
Introduction
Large bone defects, often stemming from trauma, tumors, or infections, represent a formidable challenge in orthopedic clinical practice. Current reliance on autologous bone transplantation is frequently hampered by limited bone supply and the inherent risk of donor site morbidity1. This challenge is amplified in osteoporotic elderly patients, where bone defects often culminate in fracture non-union, compounding treatment complexity due to the reduced efficacy of autologous grafts. Consequently, the development of artificial bone replacement materials with superior biocompatibility, osteoconductivity, osteoinductivity, and anti-aging/anti-osteoporotic capabilities is critically needed for effective bone defect repair2. In earlier studies, our group successfully developed an alpha-calcium sulfate hemihydrate/nano-hydroxyapatite (α-CSH/n-HA) composite3,4 by exploiting the synergistic properties of its components. Nevertheless, the osteogenic and angiogenic properties of such a composite proved unsatisfactory, consistent with existing literature5,6.
Quercetin, a 3,5,7,3′,4′-pentahydroxy flavonoid, is extensively investigated due to its association with reduced disease incidence7,8 and its prominence as an active component in herbal medicines9,10. Recent findings by Rajalakshmi S et al.11 and Lucia Forte et al.12 demonstrate that quercetin and its derivatives possess significant osteogenic-inducing and angiogenic properties, crucially promoting bone marrow mesenchymal stem cell (BMSC) osteogenic differentiation. Given that BMSCs are multipotent stem cells13 whose proliferation, migration, and differentiation capabilities are pivotal for bone defect repair14,15, these findings are highly relevant. The intricate process of in vivo bone injury repair can be reliably simulated using experimental bone defect models16. The “Critical-Size Bone Defect” (CSD) criterion17, characterizing defects incapable of spontaneous healing18, is widely adopted for animal models. Specifically, Ribeiro and Melo19 established that a 3 × 4 mm unilateral bone cortex defect in the upper tibia of SD rats constitutes a “critical bone defect.” This well-characterized “critical bone defect” model of the rat upper tibia has been consistently employed across our research group’s studies3.
Inspired by recent findings12, this project innovatively integrated quercetin into an α-CSH/n-HA scaffold. Our primary objectives were to refine the preparation method for this novel Q-α-CSH/n-HA composite, systematically evaluate the influence of varying quercetin concentrations on its physicochemical properties in vitro, and identify the optimal quercetin content. Acknowledging the significant anti-aging effects of quercetin, we established two distinct critical tibial bone defect models. We utilized the Q-α-CSH/n-HA composite as a filling material in both 8-week-old (young) male and 1-year-old (old) female SD rats. The study aimed to assess the ability of the composite in repairing bone defects, thereby generating foundational data for future clinical investigations and validating the scientific rationale for expanding the clinical utility of Q-α-CSH/n-HA.
Methods
Laboratory materials
Cylindrical samples of Q-α-CSH/n-HA composite (3 × 5 mm, diameter×height) containing 0%, 0.5%, 1.5%, or 3% quercetin (w/w to solid) were prepared. The specific Q-α-CSH/n-HA complex utilized in this study was synthesized as previously described by our research group3, noting that the physicochemical properties of the resulting compounds varied with different quercetin ratios. The preparation method involved combining α-CSH and n-HA powders at a mass ratio of 6:4, followed by mixing with quercetin at the specified ratios to yield the composite material. Sterilization was achieved via Co60 irradiation at a dose of 25 K (technical support: Guangzhou Huada Biotechnology Co., LTD.).
Physicochemical characterization of the Q-α-CSH/n-HA composite
With support from the Department of Materials Science and Engineering, School of Chemistry and Materials, Jinan University, we performed comprehensive physicochemical characterization of the Q-α-CSH/n-HA composite. To assess degradation, Q-α-CSH/n-HA and α-CSH/n-HA composites were immersed in a degradation liquid. FTIR and energy-dispersive x-ray (EDX) analysis were then utilized to examine the elemental composition and released content of both the composite materials and the degradation liquid, comparing degraded and undegraded samples.
Fourier transform infrared spectroscopy (FTIR)
The chemical structure of the novel Q-α-CSH/n-HA composites, encompassing both undegraded and degraded powders, was characterized via FTIR spectroscopy. Spectra were acquired using a Bruker Vertex 70 FTIR spectrometer interfaced with a PC running dedicated analysis software. Samples were prepared by grinding and mixing with KBr, followed by pressing into thin slices for direct placement in the IR laser beam20. All spectra were collected in transmittance mode, involving 40 scans across the 400–4000 cm− 1 range. For data analysis and visualization, Origin 8.0 software was employed, with 32 spectral scans performed for each sample group.
Scanning electron microscopy (SEM)
SEM was employed to analyze powders of α-CSH/n-HA and Q-α-CSH/n-HA (0.5%, 1.5%, 3% quercetin). After mechanical grinding, representative regions of each sample were identified via SEM. Subsequently, EDX analysis was performed at two randomly selected points within a 5000× magnified visual field to quantitatively assess the chemical elemental composition, atomic concentration, and weight concentration for each experimental group.
In vitro determination of calcium ion and Quercetin concentrations
To quantify the in vitro release of calcium ions and quercetin from the composite material, the sample powder was analyzed. Inductively coupled plasma mass spectrometry (ICP-MS) was used for calcium ion determination, while liquid chromatography with tandem mass spectrometry (LC-MS/MS) was employed for quercetin concentration.
In vivo animal studies
Laboratory animals: This study utilized 40 healthy SPF-grade Sprague-Dawley rats: 12-month-old females (weighing 180–200 g) and 8-week-old males, supplied by Jinan Pengyue Experimental Animal Breeding Co., LTD. All animals were housed under SPF conditions at the Animal Experiment Center of Southern Hospital, Southern Medical University (Guangzhou, China). All animal handling and disposal conformed to the ethical guidelines established by the Animal Experiment Center of Southern Medical University.
Bone mineral density assessment
Prior to creating the tibia critical-size defect, bone mineral density (BMD) was assessed in three 8-week-old male (young) and three 1-year-old female (old) SD rats using dual-energy X-ray absorptiometry (Lunar Prodigy, Germany). Rats were anesthetized, positioned ventrally, and scanned. Regions of interest for BMD (g/cm²) determination included the spine, right tibia, and skull21.
Once the osteoporotic condition of the 1-year-old female (old) SD rats was confirmed, the 40 experimental SD rats were randomized into four distinct groups. Prior to surgery, all animals received a 1-week adaptive feeding regimen. A single surgical team performed all procedures to ensure consistency.
Design of experimental groups
Following the establishment of a right superior tibial bone defect, different bone graft replacement materials were implanted. Tibia samples were subsequently harvested at two time points: 4 and 8 weeks post-implantation. For each time point and experimental group, five rats were randomly selected, euthanized, and their specimens collected (Table 1).
Animal model establishment and surgical procedure
The critical bone defect model of the unilateral tibial cortex in rats, described by Melo and Ribeiro19,22, was adopted for this study. Anesthesia was induced via intraperitoneal injection of pentobarbital (Nembutal, 3.5 mg/100 g). A 1.5–2.0 cm straight incision, extending from the lower lateral patellar ligament to the mid-tibia, exposed the right posterior tibia. The tibialis anterior muscle membrane was incised and longitudinally dissected. A 3 mm diameter high-speed trephine bur (Fine Science Tools, USA) was then employed to create a precisely defined 3 × 5 mm cortical bone defect approximately 1 cm distal to the tibial plateau. In total, 40 critical-sized tibia defects were created and filled with the appropriate sterilized columnar Q-α-CSH/n-HA experimental material, as per the experimental grouping. Material seating was confirmed, the surgical site irrigated with sterile normal saline, and the incision closed in layers with absorbable sutures.
Postoperative care and specimen collection
Post-surgically, the recovery of the experimental rats was closely observed, with baseline vital parameters such as heart rate, core body temperature, and respiratory rate meticulously recorded. On the second day following the surgical procedure, routine dressing replacements were conducted, concomitantly with assessments of wound healing progression. Subsequently, rats were provided with a standard pellet diet (containing 1.20% calcium and 0.92% phosphorus) for routine sustenance. At both 4 and 8 weeks post-operation, the rats within each experimental group were humanely euthanized via an intraperitoneal overdose injection of pentobarbital. The right tibias were then carefully harvested, with the peritibial soft tissue meticulously excised. Gross examination was performed to assess the healing status of the bone defect area and identify any signs of infection or pathological fracture. All collected specimens were initially fixed in a 4% paraformaldehyde solution buffered by 0.1 M phosphate (pH 7.2) for a duration of 24 h, prior to transfer into 70% ethanol for continued preservation pending further analysis.
Imaging analysis
X-ray radiography
A Faxitron X-ray system (Model: MX-20, Faxitron X-ray Corporation, Tucson, Arizona, USA) was employed for two-dimensional radiographic imaging. This imaging served two primary purposes: to confirm the correct position of bone defects and implanted materials immediately after surgery, and to assess the progression of bone defect healing at 4 and 8 weeks post-operation.
Micro-computed tomography (micro-CT) analysis
Following gross specimen harvesting of tibias at 8 weeks post-surgery, micro-computed tomography (micro-CT) was performed for detailed evaluation of bone repair within the defect area and for comprehensive bone morphological analysis. All specimens were fixed in 4% formaldehyde for 24 h prior to examination with a µ-CT system (Guangzhou Zhongke Kaisheng Medical Technology Co., Ltd.), operating at 60 W power and a maximum voltage of 50 KVp. For quantitative analysis, a fixed region of interest (ROI) with a 2.0 mm surrounding diameter was delineated along the long axis of the tibia to calculate bone volume/total volume (BV/TV, %).
Bone mineral density (BMD) analysis
Three-dimensional images were reconstructed using Med-Project software. Within the defined ROI for four animals per group, the following morphometric parameters were quantitatively assessed: BMD (mg/cm3), bone volume/total volume (BV/TV, %), trabecular separation/spacing (Tb.Sp, µm), trabecular thickness (Tb.Th, µm), and trabecular number (Tb.N, 1/mm).
Morphological analysis of specimens
Following 4 and 8 weeks of implantation, tibial segmental defect specimens were harvested for histological analysis. Tissue specimens underwent decalcification in 10% EDTA for 28 days, followed by graded dehydration through 70%-100% ethanol, and subsequent paraffin embedding. Four-µm sections were then cut from the paraffin blocks. These paraffin sections were subjected to standard deparaffinization and gradient ethanol rehydration protocols. Sections were subsequently stained with hematoxylin and eosin (H&E), Goldner trichrome, and Safranin O. Examination of stained sections was performed using an Olympus U-RFLT50 fluorescence microscope (Japan). Quantitative analysis of H&E, Goldner trichrome, and Safranin O-stained slides from each group was conducted using ImageJ software (Version 1.4). The proportion of newly formed bone volume (NBV/ROI, %), newly formed cartilage volume (NCV/ROI, %), and the blank region (BR/ROI, %) within the defined ROI were determined according to the following formulas:
NBV/ROI (%)=(NBV/ROI)×100; NCV/ROI (%)=(NCV/ROI)×100; BR/ROI (%)=(BR/ROI)×100. An experienced pathologist independently evaluated all these results. Descriptive statistics were provided as mean ± standard deviation (SD). Pairwise comparisons and within-group analyses were conducted using the t-test.
Immunofluorescence staining
Immunofluorescence (IF) staining was performed to assess the expression of runt-related transcription factor 2 (RunX2), osterix (OSX), and osteocalcin (OCN). Stained sections were visualized under a fluorescence microscope. Quantitative analysis of the IF-stained samples, performed on N = 3 biological replicates per group, was conducted using ImageJ software (Version 1.4). All findings were independently validated by an experienced pathologist.
Determination of serum calcium ion and quercetin concentrations
When tibia specimens were harvested at 4 weeks postoperatively, serum samples (from 5 rats per group) were simultaneously collected for the determination of Ca2+ and quercetin concentrations. Ca2+ levels were assessed using ICP-MS (IRIS Intrepid IIXUV, Thermo Fisher Scientific, Waltham, USA), while quercetin concentrations were measured by LC-MS/MS (Agilent Technologies, USA), as detailed previously23. The Department of Materials Science and Engineering, School of Chemistry and Materials, Jinan University, provided laboratory assistance for this work.
Colony-forming unit (CFU) assay
BMSC recruitment in Q-α-CSH/n-HA-induced bone defects was assessed via a colony-forming unit (CFU) experiment. Both in vitro and in vivo experiments indicated a superior osteogenic potential and bone defect repair efficacy for the 3% Q-α-CSH/n-HA group, thereby α-CSH/n-HA and 3%Q-α-CSH/n-HA groups (old rats) were chosen for the CFU study (Table 2). The rat right superior tibia critical bone defect model, detailed in the “Animal Experiments” section, was employed. Two weeks post-surgery, specimens were harvested for CFU analysis. After isolating and PBS-washing rat tibias, the bone marrow cavity was flushed with low-sugar medium to collect bone marrow solution. This solution was incubated at 37℃, with a medium change at 48 h. BMSC identification was confirmed by microscopic observation of cell morphology. Finally, BMSCs were seeded into solid culture dishes, cultured for 48 h, and their growth status monitored.
Statistical analyses
All statistical analyses were conducted with SPSS version 21.0 software (SPSS Inc., USA). Data were expressed as the mean ± SD. Comparisons among multiple groups were performed using one-way analysis of variance (ANOVA) with subsequent Tukey-Kramer post hoc testing. Statistical significance was defined as a P value < 0.05.
Results
FTIR analysis of the Q-α-CSH/n-HA composite
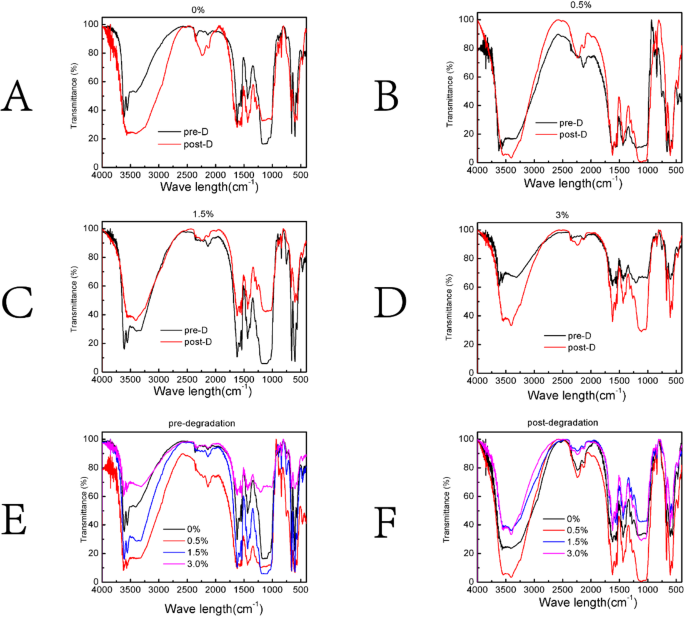
Figure 1A-F illustrates the FTIR spectra of the composites. Characteristic O-H stretching vibrations of α-CSH appeared between 3400 and 3500 cm− 1, while S-O stretching vibrations were noted at 600–680 cm− 1 and 1110–1150 cm− 1. The presence of n-HA was confirmed by phosphate peaks at 990–1000 cm− 1. The addition of quercetin led to an increase in absorption peak intensity within the 3100–3600 cm− 1 range. Following degradation, a significant decrease in peak intensity was observed for Q-α-CSH/n-HA at both 3400–3500 cm− 1 and 1000–1200 cm− 1 compared to undegraded counterparts. This phenomenon was especially prominent in the 0% and 3% Q-α-CSH/n-HA groups, yet negligible in the 0.5% group, with the 1.5% group exhibiting an inverse pattern. The undegraded composites generally showed a consistent intensity order at 3400–3500 cm− 1 and 1000–1200 cm− 1 (0.5%, 1.5%, 0%, 3% quercetin). A similar, though distinct, order was observed for degraded Q-α-CSH/n-HA (0.5%, 0%, 1.5%, 3% quercetin) (Fig. 1A-F).

Fourier transform infrared (FTIR) spectra of Q-α-CSH/n-HA composites with varying quercetin concentrations. (A-D) FTIR spectra for 0%, 0.5%, 1.5%, and 3% Q-α-CSH/n-HA composites, shown before and after degradation. (E-F) A comparative representation of the composites, illustrating the effects of degradation across all quercetin concentrations.
SEM analysis
The undegraded Q-α-CSH/n-HA composites, across quercetin concentrations of 0%, 0.5%, 1.5%, and 3%, exhibited no significant differences in the composition of their primary elements. Calcium (10.2–40.7%), sulfur (2.2–29.6%), and oxygen (26.9–73.6%) remained the most abundant. Intriguingly, higher quercetin concentrations led to an increased diversity and complexity of elemental species. Prior research indicates n-HA particle sizes of approximately 50 μm. Morphologically, SEM images (Fig. 2A-H) revealed no significant differences between undegraded α-CSH/n-HA and Q-α-CSH/n-HA (0.5%, 1.5%, 3%) powders. Post-degradation, the Q-α-CSH/n-HA composite displayed an increase in voids, greater exposure of microspheres, and a reduction in rod-like crystal structures.

Scanning electron microscopy (SEM) of Q-α-CSH/n-HA composites before and after degradation. (A-D) Illustrations represent the morphology of α-CSH/n-HA (A), 0.5% Q-α-CSH/n-HA (B), 1.5% Q-α-CSH/n-HA (C), and 3% Q-α-CSH/n-HA (D) prior to degradation. (E-H) Images show the corresponding morphology of α-CSH/n-HA (E), 0.5% Q-α-CSH/n-HA (F), 1.5% Q-α-CSH/n-HA (G), and 3% Q-α-CSH/n-HA (H) following degradation.
BMD results
As shown in Fig. 3A, the mean BMD values for the spine, tibia, and skull differed significantly between old (12-month-old female) and young (8-week-old male) rats. Specifically, old rats had significantly lower BMD values across all regions: spine (0.122 ± 0.01 g/cm2 vs. 0.154 ± 0.01 g/cm2), tibia (0.143 ± 0.01 g/cm2 vs. 0.174 ± 0.01 g/cm2), and skull (0.131 ± 0.01 g/cm2 vs. 0.161 ± 0.01 g/cm2) (P < 0.001).

Assessment of bone mineral density (BMD) in rats and elemental/quercetin content of Q-α-CSH/n-HA composites. (A) BMD values obtained from the spine, right tibia, and skull regions of both young (8-week-old male) and old (12-month-old female) rats. (B) Calcium ion content within the extracts of 0%, 0.5%, 1.5%, and 3% Q-α-CSH/n-HA. (C) Quercetin content present in the extracts of 0.5%, 1.5%, and 3% Q-α-CSH/n-HA composites. (D-E) Representative X-ray photographs of the tibia acquired immediately following composite transplantation. Statistical significance: *P < 0.05; **P < 0.01; ***P < 0.001.
Calcium ion and quercetin concentrations in Q-α-CSH/n-HA
The concentrations of calcium ions (Ca2+) and quercetin within the Q-α-CSH/n-HA complex were systematically analyzed. The measured Ca2+ concentrations in the composite extracts across all experimental groups ranged from 67.3 to 82.5 µg/mL, with statistically significant variations observed between the groups. Furthermore, the concentration of quercetin in the composite extracts exhibited a direct correlation with the increasing initial quercetin mass ratio incorporated into the Q-α-CSH/n-HA composite. Statistically significant differences in quercetin concentration were observed among the 0.5% (50.4 ± 2.36 ng/mL), 1.5% (81.23 ± 1.66 ng/mL), and 3% (92.38 ± 1.65 µg/mL) groups (Fig. 3B, C).
Post-transplantation X-ray radiography of the tibia
Radiographic analysis confirmed the successful creation of all critical tibia defect models. The blank control group consistently exhibited well-defined, low-density bone defects in the upper tibia, characterized by neat shapes and ideal anatomical positioning. In contrast, all implanted scaffold materials within the experimental groups appeared as bright white, high-signal radiopacities with clear boundaries, demonstrating X-ray densities significantly exceeding that of the adjacent normal bone. Furthermore, X-ray films of 12-month-old female SD rats visibly demonstrated significantly reduced tibial bone density, indicative of severe osteoporosis, a finding corroborated by their measured BMD values (Fig. 3D, E).
Postoperative survival analysis
Following anesthesia, all SD rats exhibited normal recovery, characterized by restored spontaneous breathing, routine feeding, and typical activity levels. The surgical incision sites demonstrated excellent Class I healing, entirely free of erythema, exudate, or purulent discharge. Suture absorption was complete around 7 days post-surgery, precluding the need for removal. Importantly, no postoperative infections were observed throughout the study.
Gross morphology and X-ray analysis at 4 and 8 weeks post-operation
A notable complication observed during harvest in all old rat groups was the occurrence of fractures at the modeling site, attributed to severe osteoporosis and brittle bone. Gross examination of tibial specimens at 4 weeks post-operation revealed no instances of hyperostosis (Fig. 4A). By 8 weeks post-operation, a single case of pseudarthrosis formation at the tibial modeling site was noted exclusively in the 3% Q-α-CSH/n-HA group, accompanied by compensatory fibular hypertrophy. Across all groups, no fibula fractures, infections, or foreign body reactions were identified surrounding the modeling area. However, the overall condition of the bone defect, periosteum, and soft tissue was generally fair (Fig. 4B).

Gross specimen morphology and X-ray examination at 4 and 8 weeks postoperatively. (A) Gross specimen morphology and X-ray images of the tibia at 4 weeks post-operation. The images highlight early bone remodeling within the defect area and the degradation and absorption of the implanted Q-α-CSH/n-HA composite for each group. (B) Gross specimen morphology and X-ray images of the tibia at the 8-week post-operative time point, detailing the further progression of bone remodeling, as well as material degradation and absorption in each experimental group.
Micro-CT analysis of bone morphology
Micro-CT analysis was performed on old rat tibial specimens at 8 weeks post-modeling to assess bone defect repair and implant degradation across experimental groups. The α-CSH/n-HA group demonstrated substantial implant absorption, with only trace material residue evident on CT scans. Remarkably, the three Q-α-CSH/n-HA groups exhibited significantly enhanced bone defect repair efficacy compared to the α-CSH/n-HA group. Among all treatments, the 1.5% Q-α-CSH/n-HA group showed the most favorable critical bone defect repair; nevertheless, CT reconstructions still revealed a discernible bone defect area and a significant amount of residual implant material within the repair region (Fig. 5A).

Micro-computed tomography (micro-CT) analysis of tibial specimens at 8 weeks post-transplantation of Q-α-CSH/n-HA composite. (A) Representative micro-CT scanning images of tibias, illustrating the extent of bone defect repair and composite integration. (B-F) Quantitative representations of bone morphometric parameters derived from micro-CT data: (B) bone mineral density (BMD, mg/cm3); (C) bone volume/total volume (BV/TV, %); (D) trabecular thickness (Tb.Th, µm ); (E) trabecular number (Tb.N, 1/mm); (F) trabecular separation (Tb.Sp, µm). The red line displays the height of the horizontal cross-sectional scan used for analysis. Statistical significance: *P < 0.05; N.S., not statistically significant (P ≥ 0.05).
Data obtained from the ROI in micro-CT scans of old rat tibia specimens were statistically analyzed (Fig. 5B-F; Table 3). While BMD, BV/TV (%), and Tb.N generally showed similar trends, only the 3% Q-α-CSH/n-HA group demonstrated a significant increase in these parameters compared to the α-CSH/n-HA group (P < 0.05) (Fig. 5B, C,E). Furthermore, increasing quercetin concentration correlated with an upward trend in Tb.N and Tb.Th, and a downward trend in Tb.Sp (Fig. 5D, E,F).
Histopathological staining analysis
Consistent findings were observed across H&E, Goldner trichrome, and Safranin O staining (Figs. 6 and 7). At 4 weeks post-operation, α-CSH/n-HA and 0.5% Q-α-CSH/n-HA groups demonstrated obvious bone defects, characterized by low numbers of chondrocytes and osteoblasts, loose bone structure, and minimal tissue infiltration (Fig. 6A-C). In contrast, the 3% Q-α-CSH/n-HA group showed a higher proportion of chondrocytes and osteoblasts, significantly reduced bone defect area, and superior repair.

Histological and quantitative analysis of tibial defect repair at 4 weeks post-transplantation. (A-C) Representative images from hematoxylin and eosin (H&E) staining (A), Goldner trichrome staining (B), and Safranin O staining (C). (D) Newly formed bone volume/region of interest (NBV/ROI, %). (E) Newly formed cartilage volume/region of interest (NCV/ROI, %). (F) Blank region/region of interest (BR/ROI, %). Statistical significance is denoted by: *P < 0.05; N.S., Not statistically significant (P ≥ 0.05). Red arrows represent chondrocytes, blue arrows represent osteoblasts, and green arrows represent new blood vessels.

Histological and quantitative analysis of tibial defect repair at 8 weeks post-transplantation. (A-C) Representative images from hematoxylin and eosin (H&E) staining (A), Goldner staining (B), and Safranin O staining (C). (D-F) Quantitative histomorphometric analyses: NBV/ROI (%) (D), NCV/ROI (%) (E), and BR/ROI (%) (F). Statistical significance is denoted by: *P < 0.05; N.S., Not statistically significant (P ≥ 0.05). Red arrows represent chondrocytes, blue arrows represent osteoblasts, and green arrows represent new blood vessels.
By 8 weeks, all four groups exhibited increased chondrocyte populations relative to 4 weeks, with chondrocyte numbers increasing proportionally with quercetin concentration in the Q-α-CSH/n-HA complex. The α-CSH/n-HA group still presented a noticeable bone defect, albeit significantly smaller than at 4 weeks (Fig. 7A-C). The 3% Q-α-CSH/n-HA group achieved a significantly smaller defect area, displaying extensive neovascularization, chondrocytes, and osteoblasts, indicative of the most effective repair. Quantitative analyses of NCV/ROI mirrored NBV/ROI. Both NCV/ROI and NBV/ROI showed a clear increasing trend with elevated quercetin concentration in the composite. Conversely, BR/ROI decreased, reaching its lowest value in the 3% Q-α-CSH/n-HA group (Figs. 6D-F and 7D-F).
Immunofluorescence analysis at 8 weeks
Immunofluorescence staining at 8 weeks post-surgery quantified RunX2, OSX, and OCN expression in rat tissues. In the α-CSH/n-HA group, positive cells for these markers were scarce and limited to the bone defect repair surface. Conversely, increasing quercetin concentration significantly augmented the number of positive RunX2, OSX, and OCN cells. The 3% Q-α-CSH/n-HA group showed the most abundant positive cells, primarily distributed in newly formed bone trabecular spaces, medullary spaces, and perivascular regions around capillaries, often forming nested or honeycomb-like structures (Fig. 8A-F).

Immunofluorescence and quantitative analysis of osteogenic markers at 8 weeks post-Q-α-CSH/n-HA transplantation. (A-C) Immunofluorescence staining for RunX2 (A), OSX (B), and OCN (C) in old rat tibias. (D-F) Quantitative comparison of positive cells for RunX2 (D), OSX (E), and OCN (F) across different groups. Statistical significance: *P < 0.05. Green fluorescence labels RunX2-positive cells, while blue fluorescence (DAPI) highlights nuclei.
Serum calcium and quercetin concentrations
Figure 9A, B presents the statistical analysis of serum calcium ion and quercetin concentrations in experimental rats. We observed an increasing trend in serum calcium ion concentration with higher composite quercetin content; the α-CSH/n-HA group had the lowest value (67.32 ± 10.45 µg/mL), while the 1.5% Q-α-CSH/n-HA group had the highest (82.41 ± 13.46 µg/mL). However, these inter-group differences were not statistically significant (P > 0.05). In parallel, serum quercetin concentration also increased with increasing quercetin content in Q-α-CSH/n-HA. Pairwise comparisons showed that both the 1.5% (81.36 ± 4.658 ng/mL) and 3% (92.74 ± 7.521 ng/mL) Q-α-CSH/n-HA groups had significantly higher concentrations than the 0.5% Q-α-CSH/n-HA group (50.39 ± 3.354 ng/mL) (P < 0.01). While quercetin generally tended to elevate serum calcium ion levels, the observation that the 3% Q-α-CSH/n-HA group had a slightly lower serum calcium ion concentration than the 1.5% group, despite higher quercetin, suggests that high quercetin concentrations might increase calcium ion absorption by surrounding tissues. As this difference was not statistically significant, it could be an incidental finding. Further experiments are necessary to definitively establish the influence of quercetin on systemic calcium ion concentrations.

Serum ion concentrations and in vitro BMSC colony formation. (A) Serum calcium ion (Ca2+) concentration in rats at 4 weeks after operation. (B) Serum quercetin concentration in rats at 4 weeks after operation. (C) Results of the in vitro BMSC clonal colony formation assay from SD rats. Statistical significance: *P < 0.05; N.S., Not statistically significant (P ≥ 0.05).
BMSC colony formation induced by Q-α-CSH/n-HA
To investigate the differential capacity of α-CSH/n-HA versus quercetin-containing Q-α-CSH/n-HA to recruit BMSCs within the bone defect repair zone of SD rats, we extracted BMSCs and performed in vitro assays. Our analysis focused on the clonal colony formation capacity induced by the two materials. The 3% Q-α-CSH/n-HA group exhibited a significantly higher number of colonies (20 ± 3.87) compared to the α-CSH/n-HA group (8.56 ± 1.53) (P < 0.05) (Fig. 9C).
Discussion
The fundamental principle of FTIR spectroscopy involves the analysis of characteristic infrared spectra generated by the interaction of interference light with a sample, thereby enabling the determination of the material sample internal structure. In the context of our spectral analysis, our results suggest that in vitro degradation of the 1.5% Q-α-CSH/n-HA composite led to the release of more active hydroxyl, amino, and sulfate groups, implying enhanced in vitro bioactivity and potential in vivo effects. Although increasing quercetin content diversified the elemental composition, no significant deviation was observed in the chemical group content within the relevant spectral range. Ca2+ content fluctuated considerably among different Q-α-CSH/n-HA groups, while quercetin content increased directly with its initial ratio in the composite. We speculate that the continuous biodegradation and quercetin release from the implanted Q-α-CSH/n-HA composite create a localized high-concentration quercetin microenvironment within the bone defect, thereby accelerating bone repair and reconstruction.
Our histopathological staining demonstrated a marked increase in the formation of ordered, widely distributed new trabecular bone in the modeling area of the Q-α-CSH/n-HA composite group, a significantly better outcome than in the α-CSH/n-HA and control groups. This strongly suggests that quercetin incorporation significantly enhances new bone formation and bone defect repair. Furthermore, the Q-α-CSH/n-HA composite exhibited excellent in vivo biocompatibility. While the reabsorption of most absorbable bone replacement materials typically initiates concurrently with the creeping substitution of new bone, with absorption and osteogenic repair proceeding in parallel24, a marked divergence was observed in our experiment. Specifically, the degradation and absorption rate of the material in the α-CSH/n-HA group was found to be more rapid than the rate of new bone growth. In contrast, the Q-α-CSH/n-HA composite group presented a fundamentally different regenerative milieu, characterized by an extensive neovascularization network and newly formed bone trabeculae permeating and intricately interweaving throughout the entire material implantation area, a phenomenon closely mirroring the patterns of trabecular bone regeneration reported by Nilsson et al.25. We propose that the combined presence of n-HA and quercetin, along with microporous structures generated by α-CSH degradation and absorption, served to attract BMSCs. These BMSCs migrated and attached within the composite, subsequently differentiating into osteoblast progenitors, maturing into osteoblasts, and undergoing progressive mineralization to form new bone trabeculae. This mechanism represents a significant departure from the creeping substitution observed with α-CSH/n-HA. Our data suggest that quercetin fundamentally alters bone defect repair, transforming it from a mere creeping substitution into a more complex process involving material-cell interactions (mechanization), neovascularization, BMSC migration, proliferation, and osteogenic differentiation. This kind of bone defect repairing from the inside and the creeping substitution from the outside of the material together constituted the novel whole process of bone defect repairing of the Q-α-CSH/n-HA composite.
RunX2, a critical downstream target of the Smads signaling pathway26, plays a pivotal role in osteogenesis. It upregulates early osteogenic markers, including OCL I and BMP-227, and promotes the expression of late differentiation genes such as alkaline phosphatase (ALP) and osteocalcin28. We also examined Osterix (OSX), another essential osteogenic transcription factor within the SP/XKLF family29. OSX is intimately involved in BMSC osteogenic differentiation and bone formation, showing bone tissue-specific expression during development30 and responsiveness to BMP-2. Osteocalcin (OCN), an abundant non-collagenous protein secreted primarily by mature osteoblasts, is a reliable marker of osteoblast maturation and significantly influences osteoblast morphology31. Furthermore, Runx2 is known to regulate OCN expression by binding to a specific response element (OSE2) in the OCN promoter region32.
Our immunofluorescence analysis revealed a significant, dose-dependent increase in RunX2-, OSX-, and OCN-positive cells within the bone defect tissue corresponding to elevated quercetin concentrations. While serum calcium ion concentration also trended upwards with increasing quercetin, this difference was not statistically significant. Serum quercetin concentration, however, significantly increased with composite quercetin content. These observations strongly suggest that quercetin acts as a key modulator, upregulating RunX2, OSX, and OCN gene expression in BMSCs. Prior studies have consistently reported that quercetin promotes the proliferation and osteogenic differentiation of BMSCs in a concentration-dependent manner, concurrently upregulating the expression of genes such as OSX, Runx2, and OPN33. We posit that the RunX2 and OSX transcription factors, situated upstream in the osteogenic differentiation signaling pathway, play a pivotal role in mediating the quercetin-induced promotion of BMSC osteogenic differentiation. These mechanistic insights are largely consistent with recent advancements in the field33. Furthermore, in vivo evidence demonstrating that oral gavage treatment with quercetin enhances bone healing after bone allograft in rats with tibial defects provides additional validation for the therapeutic effect of quercetin34. While quercetin and associated metal ions, especially calcium ions, constitute the principal active substances released upon composite degradation and are acknowledged for their significant regulatory roles in both osteogenesis and angiogenesis during bone defect repair35, the observed alterations in RunX2, OSX, and OCN gene expression in this particular study may not be directly attributable to changes in calcium ion concentration.
The well-established therapeutic applicability of quercetin has stimulated extensive investigations into its underlying mechanisms of action. Previous studies have demonstrated that quercetin can activate the Wnt/β-catenin signaling pathway through microRNA (miRNA) mediation, thereby influencing the osteogenic differentiation of BMSCs36. Additionally, it has been shown to attenuate BMSC senescence and enhance osteogenic differentiation by modulating the RNA-sensing pathway activated by repetitive elements (REs)37. Furthermore, quercetin can impact the expression of downstream factors (e.g., OSX and Runx2) within the BMP signaling pathway in BMSC cells via the estrogen pathway33. Based on the compelling results of the current study, it can be reasonably speculated that quercetin composite materials mediate the observed bone defect repair by activating the BMP signaling pathway in rats. Consequently, the precise regulatory mechanism of quercetin composite materials on bone defects should be further elucidated and verified through subsequent experiments utilizing established BMSC cell lines or in vivo animal models.
The dynamic interaction between biomaterials and BMSCs is a determinant factor in the successful repair and reconstruction of bone defects38. Individually, α-calcium sulfate hemihydrate (α-CSH) and nano-hydroxyapatite (n-HA) each possess inherent biological advantages39,40. The strategic combination of these two materials allows for a synergistic integration of their respective characteristics, resulting in a composite that exhibits robust biocompatibility coupled with both osteoinductive and osteoconductive properties. Numerous investigations have previously reported the successful application of α-CSH/n-HA composite scaffolds in the context of bone defect repair41. Furthermore, evidence suggests that composite scaffolds incorporating therapeutic agents can achieve superior clinical outcomes compared to their undoped counterparts. Consequently, in the present study, quercetin was systematically introduced into the α-CSH/n-HA scaffold system. The incorporation of quercetin demonstrably enhances the physical characteristics of the composite scaffold, improves the bioavailability of quercetin, and confers substantial biological activity. In the current study, the Q-α-CSH/n-HA composite significantly augmented the recruitment of BMSCs within the bone modeling region. Previous research has indicated that targeted stimulation of aging BMSCs in aged rats with quercetin can restore their mesenchymal stem cell function and considerably improve postmenopausal osteoporosis, a phenomenon that may be intrinsically linked to the regulatory effects of quercetin on estrogen production42. These collective results suggest that quercetin actively promotes the clonal colony formation of BMSCs in vivo. Furthermore, the anti-aging and bone-inductive potentials of quercetin on BMSCs may exert a cooperative influence, thereby enhancing the overall repair of bone defects. Considering that osteoporosis observed in elderly models may be precipitated by insufficient secretion of male hormones or estrogen, our findings propose that Q-α-CSH/n-HA represents an ideal artificial bone graft, particularly well-suited for elderly and frail patients presenting with severe osteoporosis. It is posited that the degradation and absorption of the Q-α-CSH/n-HA composite, the subsequent organization of tissues, the induction of blood vessel growth (angiogenesis), the mineralization activities of osteoblasts, and the eventual formation of new bone likely maintain a delicate dynamic balance; however, the precise underlying molecular mechanisms necessitate further rigorous clarification.
Conclusions
Q-α-CSH/n-HA exhibited a superior overall in vivo bone repair effect, suggesting its potential as an ideal artificial bone graft, especially for elderly and frail patients with severe osteoporosis. The underlying mechanism may involve quercetin, possibly synergizing with calcium ions, to alter the microenvironment of the modeling region. This modulation would simultaneously upregulate RunX2, OSX, and OCN expression, unleash anti-senescent potential, and induce BMSC osteogenic differentiation and mineralization, collectively promoting bone defect repair and reconstruction. Although a dynamic balance likely governs material degradation, absorption, mechanization, vascular growth, osteoblast mineralization, and new bone formation, the precise mechanisms warrant further detailed clarification.
Data availability
All data generated or analysed during this study are included in this published article.
References
-
Wang, J. et al. Biomaterials for bone defect repair: types, mechanisms and effects. Int. J. Artif. Organs. 47 (2), 75–84 (2024).
-
Oryan, A., Monazzah, S. & Bigham-Sadegh, A. Bone injury and fracture healing biology. Biomed. Environ. Sci. 28 (1), 57–71 (2015).
-
Ren, M. et al. Enhanced bone formation in rat critical-size tibia defect by a novel quercetin-containing alpha-calcium sulphate hemihydrate/nano-hydroxyapatite composite. Biomed. Pharmacother. 146, 112570 (2022).
-
Lin, J. et al. Physicochemical and biological properties of carboxymethyl Chitosan zinc (CMCS-Zn)/α-calcium sulfate hemihydrate (α-CSH) composites. Mater. Sci. Eng. C Mater. Biol. Appl. 131, 112496 (2021).
-
Qi, X. et al. Development and characterization of an injectable cement of nano calcium-deficient hydroxyapatite/multi(amino acid) copolymer/calcium sulfate hemihydrate for bone repair. Int. J. Nanomed. 8, 4441–4452 (2013).
-
Zhang, S. et al. Preparation and properties of Chitosan quaternary ammonium salt/α-calcium sulfate hemihydrate/β-tricalcium phosphate composite bone cement. Colloids Surf. B Biointerfaces. 253, 114738 (2025).
-
Riva, A. et al. Quercetin phytosome(R) in triathlon athletes: a pilot registry study. Minerva Med. 109 (4), 285–289 (2018).
-
Patel, R. V. et al. Therapeutic potential of Quercetin as a cardiovascular agent. Eur. J. Med. Chem. 155, 889–904 (2018).
-
Zahoor, M., Shafiq, S., Ullah, H., Sadiq, A. & Ullah, F. Isolation of Quercetin and Mandelic acid from aesculus indica fruit and their biological activities. BMC Biochem. 19 (1), 5 (2018).
-
Deepika, M. P. K. Health benefits of Quercetin in age-related diseases. Molecules 27 (8), 2498 (2022).
-
Vimalraj, S. et al. Mixed-ligand copper(II) complex of Quercetin regulate osteogenesis and angiogenesis. Mater. Sci. Eng. C Mater. Biol. Appl. 83, 187–194 (2018).
-
Forte, L. et al. Antioxidant and bone repair properties of quercetin-functionalized hydroxyapatite: an in vitro osteoblast-osteoclast-endothelial cell co-culture study. Acta Biomater. 32, 298–308 (2016).
-
Gao, Q. et al. Biomaterials regulates BMSCs differentiation via mechanical microenvironment. Biomater. Adv. 157, 213738 (2024).
-
Sultana, N. et al. Evaluation of biocompatibility and osteogenic potential of tricalcium silicate-based cements using human bone marrow-derived mesenchymal stem cells. J. Endod. 44(3),446-451(2018).
-
Shuai, Y. et al. OSGIN2 regulates osteogenesis of jawbone BMSCs in osteoporotic rats. BMC Mol. Cell. Biol. 23 (1), 22 (2022).
-
Nauth, A., Schemitsch, E., Norris, B., Nollin, Z. & Watson, J. T. Critical-Size bone defects: is there a consensus for diagnosis and treatment?J. Orthop. Trauma. 32 (Suppl 1), S7–S11 (2018).
-
Walsh, W. R. et al. Critical size bone defect healing using collagen-calcium phosphate bone graft materials. PLoS One. 12 (1), e0168883 (2017).
-
Ziroglu, N. et al. Modified and alternative bone cements can improve the induced membrane: critical size bone defect model in rat femur. Injury 55 (7), 111627 (2024).
-
Ribeiro, L. L., Bosco, A. F., Nagata, M. J. & de Melo, L. G. Influence of bioactive glass and/or acellular dermal matrix on bone healing of surgically created defects in rat tibiae: a histological and histometric study. Int. J. Oral Maxillofac. Implants. 23 (5), 811–817 (2008).
-
.Gani, M. A., Budiatin, A. S., Shinta, D. W., Ardianto, C. & Khotib, J. Bovine hydroxyapatite-based scaffold accelerated the inflammatory phase and bone growth in rats with bone defect. J. Appl. Biomater. Funct. Mater. 21, 22808000221149193 (2023).
-
.Li, Y., Zhang, J., Chen, L., Li, H. & Wang, J. Repair of critical-sized rat cranial defects with RADA16-W9 self-assembled peptide hydrogel. Biochem. Biophys. Res. Commun. 652, 68–75 (2023).
-
Melo, L. G., Nagata, M. J., Bosco, A. F., Ribeiro, L. L. & Leite, C. M. Bone healing in surgically created defects treated with either bioactive glass particles, a calcium sulfate barrier, or a combination of both materials. A histological and histometric study in rat tibias. Clin. Oral Implants Res. 16 (6), 683–691 (2005).
-
Lv, L. et al. Pharmacokinetics of Quercetin-loaded methoxy poly(ethylene glycol)-b-poly(L-lactic acid) micelle after oral administration in rats. Biomed. Res. Int. 2017, 1750895 (2017).
-
Ye, J. et al. Injectable, hierarchically degraded bioactive scaffold for bone regeneration. ACS Appl. Mater. Interfaces. 15 (9), 11458–11473 (2023).
-
Nilsson, K. H. et al. RSPO3 is important for trabecular bone and fracture risk in mice and humans. Nat. Commun. 12 (1), 4923 (2021).
-
Li, Z. et al. Effects of altered CXCL12/CXCR4 axis on BMP2/Smad/Runx2/Osterix axis and osteogenic gene expressions during osteogenic differentiation of MSCs. Am. J. Transl Res. 9 (4), 1680–1693 (2017).
-
Garg, P. et al. Prospective review of mesenchymal stem cells differentiation into osteoblasts. Orthop. Surg. 9 (1), 13–19 (2017).
-
Komori, T. Runx2, an inducer of osteoblast and chondrocyte differentiation. Histochem. Cell. Biol. 149 (4), 313–323 (2018).
-
Amarasekara, D. S., Kim, S. & Rho, J. Regulation of osteoblast differentiation by cytokine networks. Int. J. Mol. Sci. 22 (6), 2851 (2021).
-
Fukuda, M. et al. SIRT7 has a critical role in bone formation by regulating lysine acylation of SP7/Osterix. Nat. Commun. 9 (1), 2833 (2018).
-
Komori, T. What is the function of osteocalcin? J. Oral Biosci. 62 (3), 223–227 (2020).
-
Sanyal, S. et al. Polymorphisms in the Runx2 and osteocalcin genes affect BMD in postmenopausal women: a systematic review and meta-analysis. Endocrine 84 (1), 63–75 (2024).
-
Pang, X. G., Cong, Y., Bao, N. R., Li, Y. G. & Zhao, J. N. Quercetin stimulates bone marrow mesenchymal stem cell differentiation through an estrogen receptor-mediated pathway. Biomed. Res. Int. 2018, 4178021 (2018).
-
Durmaz, B. et al. Investigation of the effects of Quercetin and xenograft on the healing of bone defects: an experimental study. J. Oral Biol. Craniofac. Res. 13 (1), 22–27 (2023).
-
Birgani, Z. T., Gharraee, N., Malhotra, A., van Blitterswijk, C. A. & Habibovic, P. Combinatorial incorporation of fluoride and cobalt ions into calcium phosphates to stimulate osteogenesis and angiogenesis. Biomed. Mater. 11 (1), 015020 (2016).
-
Bian, W., Xiao, S., Yang, L., Chen, J. & Deng, S. Quercetin promotes bone marrow mesenchymal stem cell proliferation and osteogenic differentiation through the H19/miR-625-5p axis to activate the Wnt/β-catenin pathway. BMC Complement. Med. Ther. 21 (1), 243 (2021).
-
Sun, Y. et al. Quercetin ameliorates senescence and promotes osteogenesis of BMSCs by suppressing the repetitive element-triggered RNA sensing pathway. Int. J. Mol. Med. 55 (1), 4 (2025).
-
Zhang, H. et al. Polyhedron-like biomaterials for innervated and vascularized bone regeneration. Adv. Mater. 35 (42), e2302716 (2023).
-
Teotia, A. K. et al. Nano-Hydroxyapatite bone substitute functionalized with bone active molecules for enhanced cranial bone regeneration. ACS Appl. Mater. Interfaces. 9 (8), 6816–6828 (2017).
-
Qayoom, I. et al. Enhanced bone mineralization using hydroxyapatite-based ceramic bone substitute incorporating Withania somnifera extracts. Biomed. Mater. 15 (5), 055015 (2020).
-
Jiang, Y. et al. Asprin-loaded strontium-containing α-calcium sulphate hemihydrate/nano-hydroxyapatite composite promotes regeneration of critical bone defects. J. Cell. Mol. Med. 24 (23), 13690–13702 (2020).
-
Wang, Y. et al. Repurpose dasatinib and quercetin: targeting senescent cells ameliorates postmenopausal osteoporosis and rejuvenates bone regeneration. Bioact Mater. 25, 13–28 (2023).
Funding
This work was supported by National Natural Science Foundation of China (8227091135).
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The experimental protocols were approved by the Ethics Committee of the Sixth Afffliated Hospital, South China University of Technology, and in compliance with the Sixth Afffliated Hospital of South China University of Technology guidelines for the care and use of animals. I confirm that all methods are reported in accordance with relevant guidelines and regulation and adhered to ARRIVE guidelines.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ren, M., Yang, Y., Chen, K. et al. Bone regeneration induced by a novel quercetin/a-CSH/n-HA composite in critical size tibia defect of rats with osteoporosis. Sci Rep 15, 36273 (2025). https://doi.org/10.1038/s41598-025-20161-z
-
Received:
-
Accepted:
-
Published:
-
DOI: https://doi.org/10.1038/s41598-025-20161-z