Introduction
Craniomaxillofacial reconstruction (CMFR) is a critical domain within reconstructive surgery, addressing defects in the skull, face, and jaws caused by trauma, congenital malformations, or tumor resections.1,2,3 The craniomaxillofacial region is uniquely complex, housing vital structures such as the brain, eyes, and airways, while supporting essential functions like chewing, speech, and facial expression. Successful reconstruction demands not only structural restoration but also functional recovery and esthetic harmony to improve patients’ quality of life.4,5 Historically, CMFR relied on biological grafts—autografts (e.g., iliac crest bone), allografts, and xenografts—which offer osteoconductive and osteoinductive properties.6 However, these approaches face significant limitations: autografts cause donor site morbidity,7 allografts risk immune rejection,8 and xenografts may transmit diseases.9 These challenges, coupled with inconsistent tissue availability, have driven the development of synthetic craniomaxillofacial implants (CMFIs). CMFIs provide customizable, reproducible solutions tailored to individual anatomies, aiming to restore structural integrity, promote osseointegration, and achieve cosmetically acceptable outcomes.10
Despite the advancements, current reconstructive CMFIs encounter persistent hurdles. For example, mechanical mismatches with native bone, infection susceptibility, long-term instability of degradation, and poor osseointegration remain prevalent.11,12 The craniomaxillofacial region’s exposure to dynamic loads (e.g., masticatory forces) and its proximity to critical anatomical structures amplify these issues, necessitating innovative solutions. Next-generation CMFIs should address these shortcomings, leveraging breakthroughs in biomaterials, design architectures, manufacturing technologies. For instance, growing research interest in biomaterials has been directed toward bioactivity, including osteoinductivity and osseointegration. Novel designs closely emulate the biomechanical characteristics of native bone while ensuring long-term biocompatibility.13,14 Additive manufacturing has revolutionized CMFI fabrication, enabling complex porous architectures that enhance osseointegration, mitigate stress shielding, and reduce implant weight.15,16
This review synthesizes the state-of-the-art in the early-stage clinical translation of CMFIs in the recent years, including biomaterials selection, design architectures, additive manufacturing technologies, followed by discussion of preclinical evaluation methods and future directions of next-generation CMFIs. Significant attention is devoted to the balance and optimization of biomechanics, biocompatibility, and bioactivity (collectively referred to as the “3Bs” framework) throughout CMFIs development. Key criteria include biomechanical matching,17 no toxic or pro-inflammatory effects,18 osseointegration potential (chemical cues or coatings to encourage bone bonding).19 By examining these facets, we aim to provide a holistic understanding of how next-generation CMFIs are poised to transform CMFR, offering improved outcomes for patients worldwide.
Early-stage clinical translation and “3Bs” framework
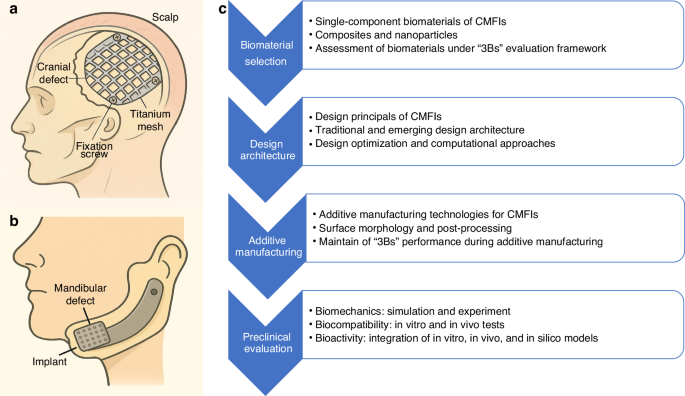
The representative examples of CMFIs are shown in Fig. 1a, b, including a titanium mesh for craniofacial reconstruction20 and an endoprosthesis for mandibular reconstruction.21 However, the clinical translation of patient-specific CMFIs requires a multi-stage process, encompassing material and design development, preclinical validation, manufacturing standardization, regulatory approval, clinical trials, and eventual market deployment and real-world implementation. This review focuses on the early-stage clinical translation, specifically addressing biomaterial selection, design architecture, additive manufacturing, and preclinical evaluation, as highlighted in Fig. 1c. Furthermore, we propose a “3Bs” evaluation framework—encompassing biomechanics, biocompatibility, and bioactivity—and advocate for its integration into the early development pipeline of next-generation CMFIs. This integration ensures next-generation CMFIs undergo comprehensive, multidimensional, and standardized evaluation throughout their development, thereby providing robust clinical support for CMFR surgery. Table 1 presents the “3Bs” evaluation framework proposed in this review, encompassing the specific indices and suggested benchmark applied to the multiscale assessment of CMFIs.

Representative examples of CMFIs and schematic overview of CMFI development. a A surgical titanium mesh used for repairing a cranial defect, showing the mesh placement and fixation with screws under the scalp. b A patient-specific endoprosthesis for mandibular reconstruction, illustrating implant positioning within the mandibular defect. c Schematic overview of the development and evaluation framework for next-generation CMFIs, highlighting the key stages: biomaterials selection, design architecture, additive manufacturing, and preclinical evaluation
Biomechanics refers to the study of mechanical principles applied to biological systems. In the context of CMFR, it encompasses the mechanical behavior of facial bones and implants under physiological loads, including stress distribution, deformation, and failure mechanisms. Maintaining or restoring biomechanical integrity is critical to the functional and structural success of CMFIs. The facial skeleton experiences complex loading conditions during mastication, speech, and expression.22 Therefore, implants must possess sufficient mechanical strength, stiffness, and fatigue resistance to withstand these forces while mimicking the native bone’s mechanical properties to avoid stress shielding or implant failure. Biomechanical optimization also plays a crucial role in long-term durability and patient-specific implants.23
Biocompatibility is defined as the ability of a material to perform its desired function without eliciting any undesirable local or systemic effects in the host. It includes cellular response, immune reaction, and toxicity.24 In CMFI applications, implants are in intimate contact with bone, soft tissue, and sometimes mucosa, making biocompatibility a fundamental requirement. Poor biocompatibility can lead to inflammation, fibrosis, implant rejection, or infection. Materials must be non-toxic, non-immunogenic, and support tissue healing.25 Moreover, high biocompatibility ensures a stable and harmonious interaction between the implant and the host environment, facilitating clinical success and patient safety.26
Bioactivity refers to the ability of a material to interact with biological tissues at the molecular level to induce specific cellular responses, such as osteogenesis, angiogenesis, or tissue regeneration. Bioactive implants not only serve as structural supports but also actively promote bone regeneration and integration.27 In CMFR, this is especially important for large or complex defects where spontaneous healing is limited. Bioactive materials can enhance osseointegration, stimulate osteoblast proliferation and differentiation, and potentially reduce healing time.28 Incorporating bioactivity into implant design represents a shift from passive materials toward regenerative solutions, aligning with the principles of tissue engineering and precision medicine.
Biomaterial selection
This section summarizes both traditional and emerging single-component and composite biomaterials, with parallel consideration given to nanomaterials—such as nanoparticles—that have also been investigated for enhancing biomaterial performance. Representative materials are evaluated with reference to the “3Bs” framework proposed in this study. Biomaterials with adequate literature support for evaluation under the “3Bs” framework are included.
Single-component biomaterials
Titanium and titanium alloys (e.g., Ti-6Al-4V), as conventional CMFIs, are backed by a comprehensive body of research and long-term clinical evidence.29,30,31,32,33,34,35,36,37 Titanium-based implants exhibit excellent strength, corrosion resistance, osseointegration and MRI-compatibility.38 However, its elastic modulus (~110 GPa) far exceeds that of cortical bone (~18–20 GPa), risking stress shielding.39 Clinically, titanium meshes and plates are standard for skull reconstruction due to their reliability, but they may require countersinking or contouring to achieve esthetic profiles.40 Furthermore, due to its non-biodegradable nature as a permanent implant material, titanium-based implant is not suitable for applications such as pediatric reconstruction and bone tissue scaffolds.41 Stainless steel has been historically used in clinical practice; their relatively lower biocompatibility and long-term stability compared to titanium have resulted in reduced usage in recent years. Emerging metal biomaterials such as magnesium alloys are biodegradable implants.38,42,43 Magnesium-based CMFIs (e.g., WE43) exhibit excellent biomechanics, as magnesium alloys have an elastic modulus more similar to that of natural bone compared to titanium alloys, thereby reducing the risk of significant stress shielding.43 Additionally, magnesium alloys enable gradual in vivo degradation and potentially eliminating the need for secondary surgical removal,42 however, controlling rapid corrosion of magnesium alloys remains a challenge. For bioactivity perspective, magnesium alloys releases magnesium ions that may stimulate bone regeneration.38
PEEK has also been widely used in clinical practice as a conventional CMFIs polymer.44,45,46,47,48 PEEK is a semicrystalline thermoplastic polymer with elastic modulus (~3–4 GPa) much closer to bone than titanium-based implants.49 Due to its chemical inertness, PEEK induces negligible inflammatory reactions and cytotoxic effects. Despite its excellent biomechanical properties and biocompatibility, PEEK lacks inherent bioactivity, which limits its ability to promote osseointegration, so surface modification (e.g., hydroxyapatite coating or plasma etching) is often explored to improve osseointegration.46 Poly methyl methacrylate (PMMA), as a traditional economical implant material, offers satisfactory mechanical performance50,51; nevertheless, its suboptimal biocompatibility and lack of bioactivity.52 Polylactide-based homopolymers and copolymers, such as Poly (L-lactic acid) (PLLA), Polylactic-co-glycolic acid (PLGA), and Poly (D, L-lactide) (PLDLLA) have been tried for pediatric CMFIs due to its biodegradability. It can provide temporary support during bone healing, then resorb over months to years. However, they generally have low strength and stiffness,53 and degradation products can induce local inflammation. Polycaprolactone (PCL) as an emerging biodegradable polymer exhibits superior biomechanical strength and slow degradation, but its relatively poor bioactivity and long-term persistence may limit its standalone use as CMFIs.54
Bioactive ceramics, such as hydroxyapatite (HA) and β-tricalcium phosphate (β-TCP), and bioactive glasses (BAG), such as 45S5 Bioglass and S53P4 Bioglass, are inherently osteoconductive or even osteoinductive.55 These materials can support bone cell attachment and stimulate new bone formation, making them highly attractive for regenerative applications.56 HA exhibits excellent biocompatibility and osteoconductivity, with a chemical composition closely resembling that of natural bone mineral, making it widely used in coatings and scaffold applications.57,58 β-TCP offers excellent osteoconductivity and biodegradability, making it suitable for resorbable bone grafts.59,60 45S5 Bioglass demonstrates excellent bioactivity and strong bonding ability to bone tissue. It degrades gradually in vivo, allowing space for new bone formation without generating toxic byproducts.61 However, bioceramics and bioglasses are brittle and typically weaker than metals and alloys, which may not meet the biomechanics requirement as the main material of reconstruction scaffold, especially in load-bearing regions. Therefore, they are more frequently utilized in composites with metals or polymers to capitalize on their superior bioactivity.62,63
Composite biomaterials and nanoparticles
Single-component biomaterials—such as metal alloys, polymers, and ceramics—each exhibit distinct advantages. Nevertheless, none of these materials alone can achieve a comprehensive balance among the “3Bs”. As a result, composite biomaterials have been extensively investigated to achieve comprehensive enhancements in the “3Bs” performance. Alloy-ceramic and polymer-ceramic composites integrate the strengths of the alloys/polymers and ceramics.64,65,66,67,68 For example, Ti6Al4V/HA combines the high mechanical strength of Ti6Al4V with the osteoconductivity of HA, promoting stable osseointegration. However, mismatch in elastic modulus and potential delamination of HA coatings may compromise long-term performance. PEEK/HA enhances the bioactivity while maintaining a bone-like elastic modulus suitable for load-bearing applications. exhibiting better cell attachment, proliferation, spreading, and higher alkaline phosphatase (ALP) activity.64 Yet, poor interfacial bonding between PEEK and HA remains a challenge for mechanical reliability. PLGA/β-TCP composites offer a balance of biodegradability and bioactivity, making them suitable for non-load-bearing CMFIs, while their limited mechanical strength and potential for acidic degradation byproducts restrict broader application. β-TCP/PLLA/PGA demonstrated significantly enhanced osteogenic cell accumulation compared to pure β-TCP, both at early and late stages of implantation.67 But similarly, its poor biomechanical property limits the reliability for load-bearing application.
Nanoparticles have been employed in CMFIs to enhance osseointegration, mechanical performance, and antibacterial properties.69 Commonly used nanoparticles include nano-hydroxyapatite (nHA) which mimics the mineral phase of bone and promotes osteogenesis70 and titanium dioxide (TiO₂) nanoparticles for surface modification and mechanical reinforcement.71 Other promising candidates include zinc oxide and silica-based nanoparticles for their osteoinductive potential, as well as bioactive glass nanoparticles that support both bone formation and angiogenesis.72 Carbon-based nanomaterials, such as graphene oxide (GO) and carbon nanotubes (CNTs), offer mechanical benefits and may regulate stem cell behavior. These nanoparticles are commonly integrated into polymer or ceramic matrices, applied as surface coatings, or incorporated into 3D-printed scaffolds to meet the complex demands of CMFR. For instance, PEEK-based bioactive composites reinforced with 0–50 vol% CaO–SiO₂ microspheres, demonstrating enhanced hydroxyapatite-forming ability and improved mechanical properties.73 TiO2 incorporated PEEK/HA also enhance the mechanical strength74 and bioactivity.75 The incorporation of nanoparticles into biocomposite systems has partially overcome the intrinsic limitations of monolithic biomaterials, thereby contributing to the enhanced “3Bs” performance in CMFIs.
Assessment of biomaterials under “3Bs” evaluation framework
A qualitative evaluation of representative CMFI implant types was conducted using the proposed “3Bs” framework, with the aim of offering preliminary clinical guidance, as detailed in Table 2. The evaluation is based on the criteria provided in Table 1. Taking titanium alloys as an example: its biomechanical performance is rated high (+++) due to its high yield strength, fracture toughness, and fatigue resistance. While a high elastic modulus can contribute to stress shielding, the value remains within an acceptable range when compared to that of stainless steel (~200 GPa), which is substantially higher and thus more prone to causing mechanical mismatch with native bone. Its biocompatibility is also rated high (+++), as the majority of clinical cases have demonstrated that titanium alloys implants are associated with minimal postoperative complications and infections. However, its bioactivity performance is relatively poor (+), since titanium alloys are intrinsically non-osteoinductive.
Design architectures
The success of CMFIs depends not only on material but also on its design architectures, such as morphology, porosity, and fixation pattern. Balancing the “3Bs” properties—biomechanics, biocompatibility, and bioactivity—is a key design principle, encompassing biomechanical matching, anatomical precision, enhancement of osseointegration, and more. Computer-aided design (CAD) accelerates the design iterations of CMFIs. Furthermore, design optimization of the CMFIs can lead to improvements in their “3Bs” performance. This section summarizes the design principles of CMFIs, emerging design architectures, and computational design workflows used to develop the CMFIs that optimize the “3Bs” performance (Fig. 2a).

Common design workflow and innovative architectural strategies of CMFIs. a Computer-aided design (CAD) workflow for CMFIs. b Representative topologies of TPMS-based scaffolds for bone reconstruction. c Rapid mechanical evaluation by adjusting porosity and pore size of the scaffolds. d Template illustrating the iterative design and optimization process of a TPMS-based scaffold aimed at minimizing stress to prevent potential structural fractures
Design principles
Given the critical role that biomechanical compatibility plays in the success of CMFIs, the design should match the biomechanical environment of the defect site. For cranial plates and jaw reconstructions, this means sufficient stiffness and strength to withstand physiological loads (e.g. masticatory forces or intracranial pressure) without fracturing, while avoiding stiffness far above native bone.76 Design strategies include thickness tuning and lattice structures to adjust stiffness. For example, finite element studies show that increasing plate thickness strongly reduces deflection under load. Conversely, introducing holes or perforations (to promote bone ingrowth) may slightly lower stiffness but often has minimal effect if geometries are optimized.11 Computational optimization (e.g. topology optimization) can tailor internal lattices so that stress distribution in an implant mimic that of bone, mitigating stress shielding. Matching fatigue behavior is also important, as jaw implants experience repeated loading; designs must avoid high-strain concentrations.77
In addition to mechanical considerations, ensuring precise anatomical conformity is also essential for optimal implant performance. Modern workflow uses patient imaging (CT/MRI) to create 3D models of the defect and contralateral anatomy.78 Techniques like mirror-imaging the unaffected side help reconstruct symmetric skull or facial features. CAD tools allow sculpting of the implant geometry for a flush fit against bone.79 Good fit reduces dead space (lowering infection risk) and improves mechanical stability by distributing load evenly. Surgical guides can be 3D-printed to ensure accurate placement of screws or osteotomies. Personalization has been shown to reduce operating time and improve outcomes.80
Another critical aspect of CMFI design is the promotion of bone ingrowth and integration. To achieve this, the surface characteristics—such as roughness, micro-porosity, and overall bulk porosity—are carefully engineered. For instance, roughened or coated surfaces (e.g., sandblasted Ti, HA coating) increase surface area and cell attachment.81 Porous internal architecture provides channels for new bone to invade.82 Designs often incorporate scaffolding regions where bone can penetrate through the implant.83 The geometry must maintain enough mechanical strength while allowing bone growth. For instance, titanium cranial implants sometimes include perforations to reduce stiffness and enable vascularization, though this must be balanced so as not to weaken the plate excessively.
Advanced design architecture in CMFIs
Introducing controlled porosity into implants can dramatically improve the 3B performance of CMFIs, as porous scaffolds reduce overall stiffness (bringing it closer to bone) and provide space for vascularized bone ingrowth.83 Common porous architectures include open-cell foams and lattices. Random or regular strut lattices (e.g., octet, cubic, or diamond truss) can be 3D printed, allowing tuning of porosity and stiffness. While simple strut lattices are straightforward to design, triply periodic minimal surface (TPMS) geometries offer continuous smooth surfaces, high surface-area-to-volume ratios, and tunable mechanical properties.84,85,86,87,88
The design parameters of TPMS structures include unit cell size (pore size), porosity, wall thickness, and topology (e.g. gyroid, diamond, primitive; see Fig. 2b). Pore size is particularly critical: larger pores enhance vascularization and bone ingrowth, whereas smaller pores increase the surface area available for cell attachment.89 In practice, intermediate pore sizes (~300–600 μm) are often selected to balance scaffold strength with osteogenic activity.90,91,92 Increasing overall porosity promotes biological infiltration but reduces stiffness, so material selection must be considered together with pore design to achieve optimal osseointegration and mechanical compatibility.93 Beyond pore size and porosity, pore shape and interconnectivity also play important roles: rounded or ellipsoidal pores reduce stress concentrations, while the smooth curvature of TPMS structures improves fatigue life.94 Because TPMS geometries are governed by mathematical functions, they can be readily generated and computationally optimized to meet balanced “3Bs” performance goals.
To illustrate the “3Bs” framework in implant design, consider three representative cases. First, 3D-printed porous Ti-6Al-4V scaffolds with well-defined circular pores and straightforward interconnected structures (pore sizes ~600 μm) were shown to achieve an optimal balance between biomechanical (mechanical properties analogous to human bone) and biological response (enhanced cell adhesion and proliferation supporting osseointegration).95 Second, modified face-centered cubic scaffolds with optimized geometry and porosity exhibited both high mechanical stiffness and efficient cell diffusion, thereby demonstrating that mathematically defined architectures can concurrently fulfill biomechanical and bioactivity requirements.96 Third, a topology-optimized titanium layered porous implant for mandibular reconstruction demonstrated that with appropriately tailored porous layout and screw fixation schemes, mechanical stability is maintained (reduced stress shielding) while also providing sufficient mechanical stimulus for bone regrowth according to mechanostat theory.97 Together, these implant cases underscore that diverse implant designs can be engineered to balance “3Bs” performance, guiding rational design toward clinical translation.
Design optimization and computational approaches
Modern CMFIs are designed using advanced computational tools. Patient imaging (CT/MRI) is first segmented to reconstruct the defect 3D geometry. CAD software Design software (often FDA-cleared platforms like Materialise or 3D Systems) enables inverse modeling or manual sculpting of the implant shape. In integrated design platforms, generative optimization algorithms can evolve an initial implant shape into an efficient structure that meets specified mechanical constraints and biological needs. Numerical simulation methods such as finite element analysis (FEA) and computational fluid dynamics (CFD) are routinely used to support the design optimization.98 FEA simulates physiological loads to predict stress distribution and implant displacement.99 In addition, CFD simulates blood flow inside the porous structure which supports osteoblast function by supplying nutrients and oxygen.100 Furthermore, the outcomes of numerical simulations can be leveraged to train predictive models using machine learning techniques, thereby significantly reducing computational costs.101 The integration of CAD, computational simulation, machine learning and numerical optimization is the future direction of structural design for CMFIs that achieve both biomechanical efficiency and biological viability.
Designing CMFIs involves navigating a multifaceted landscape of constraints and objectives tailored to patient-specific and site-specific needs, such as defect geometry, anatomical loading, and bone quality.102 For optimal biomechanical properties, the designer should find the designs that matches the elastic modulus of native bone (1–20 GPa for cortical bone, 0.1–2 GPa for cancellous bone) to minimize stress shielding.103 For enhanced biocompatibility, porosity and pore size are critical variables in the design, as they directly affect permeability and nutrient transport.100 Take cranial implants as an example, medium porosity (~50%) ensures structural integrity under intracranial pressure and allows new bone growth.104 The design of most CMFIs can be formulated as a constrained, multi-objective, continuous optimization problem—particularly when the design variables are parameterizable, as in the case of TPMS-based structures. To address the inherent trade-offs among competing objectives (the “3Bs” performance), advanced optimization techniques like genetic algorithms and Pareto-front approaches are commonly employed. These facilitate the identification of optimal design solutions that balance multiple performance criteria across diverse clinical scenarios.98,105,106
Topology optimization, morphological optimization, and size optimization have been widely applied in the CMFIs design. Topology optimization is crucial for functionally graded TPMS designs because it modifies the internal lattice structure of TPMS-based implants to optimize load distribution, weight, and biological performance.37,107,108,109,110 For example, it is reported that compared to the uniform implant, the topology-optimized implant showed 20% less stress-shielding and a 45% reduction in the mass.107 Morphological optimization adjusts the shape of the pore and hence enhanced the performance. An optimized TPMS design reduces the structural compliance by more than 10.85%, confirming the effectiveness of the proposed optimization framework for lightweight applications.111 Size optimization also plays a critical role in the design of CMFIs, particularly in refining parameters such as wall thickness and fixation configurations to enhance mechanical performance and anatomical compatibility. As an illustrative example, the optimization history of a TPMS structure demonstrates that the design converges after 21 iterations by adjusting pore size and porosity (Fig. 2c) to achieve a reduction of approximately 25% in maximum stress and 10% in average stress (Fig. 2d).
Additive manufacturing
Additive manufacturing (AM), also known as 3D printing, is a technique that builds objects layer by layer from digital models. In the field of CMFIs, AM enables the creation of highly customized implants that precisely match a patient’s anatomy. Surface treatment and post-processing techniques—such as polishing, coating, or heat treatment—are also crucial for improving the biomechanical strength, biocompatibility, and osseointegration of the implants. Together, AM and these post-processing steps ensure that CMFIs are not only anatomically accurate but also safe, durable, and effective in clinical applications. However, the inherent limitations of AM may lead to discrepancies between the actual CMFIs performance and the computational predictions. Therefore, preserving the expected “3Bs” performance throughout the additive manufacturing process is of critical importance.
AM technologies
Titanium-based implants are frequently fabricated using direct metal laser sintering (DMLS), selective laser melting (SLM) or electron beam melting (EBM). These techniques build parts layer-by-layer by selectively melting or sintering metal powder particles spread across a build platform, enabling the production of complex geometries with controlled internal porosity.112 DMLS has been effectively employed in the fabrication of patient-specific implants for the reconstruction of maxillary defects caused by mucormycosis secondary to COVID-19.113 SLM offers high resolution and has been successfully applied to manufacture patient-specific implants for 96 cases of primary orbital reconstruction. The results suggested that reconstruction in complex orbital wall fractures achieved with a high degree of accuracy by using SLM-fabricated implants.114 In addition, EBM-fabricated cranial implants have demonstrated favorable biomechanics strength and displayed a regular pattern of interconnected channels without any defects and voids, enhancing the esthetic and functional rehabilitation of craniofacial deformities with faster healing and bone ingrowth formation and achieving immediate and efficient reconstruction.104 Recent developments have shown the feasibility of AM for Mg alloys based on laser powder bed fusion (L-PBF)115 and binder jetting.116 However, the risk of combustion during Mg-Zn alloys processing and the inherent corrosion of the Mg-based alloys should also be carefully considered.117
Polymers have emerged as promising materials for 3D-printed CMFIs due to their excellent processability and tunable properties. PEEK can be processed using fused filament fabrication (FFF), also known as fused deposition modeling (FDM).118 High-temperature FFF systems are capable of melting PEEK and depositing it with precision, enabling the fabrication of implants that closely match CAD geometries. Stereolithography (SLA), selective laser sintering (SLS), and digital light processing (DLP) enable the printing of bioresorbable polymers such as PCL and PLA and have been reported to maintain the biocompatibility of CMFIs.119 Polymers can be processed using AM techniques to fabricate complex, patient-specific geometries. For example, 3D-printed PEEK implants have been successfully used in mandibular reconstruction, while PCL scaffolds loaded with growth factors promote bone regeneration in defect sites. Overall, polymer-based 3D printing enables the production of lightweight, precise, and functionally effective implants tailored to individual clinical needs.
The AM of bioceramics scaffolds is primarily accomplished via ceramic SLA/DLP, direct ink writing (DIW, or robocasting), and powder-based methods such as binder jetting. Ceramic SLA/DLP 3D printing enables the fabrication of complex, high-resolution ceramic parts by photopolymerizing a slurry composed of ceramic particles suspended in a photosensitive resin. After printing, the parts undergo sintering to achieve full ceramic density.120 In DIW, a viscous ceramic slurry—comprising ceramic particles (e.g., HA, β-TCP, or bioactive glass) suspended in a biopolymer matrix—is extruded through a fine nozzle to form predefined lattice architectures.121 The printed structure is then dried and sintered at high temperatures to remove organics and densify the ceramic, yielding porous scaffolds with controlled geometry and interconnected networks favorable for bone ingrowth. In contrast, binder jetting selectively deposits a binder onto a ceramic powder bed to form a “green” part, which is subsequently consolidated via sintering.120 In comparison to metals and polymers, the clinical translation of 3D-printed ceramic materials remains relatively limited, primarily due to challenges associated with their brittle nature, high-temperature processing requirements, and complex post-processing procedures.
Current AM-fabricated composite biomaterials for CMFIs are primarily developed using FFF (FDM), DIW, and multi-material jetting technologies. FFF is well-suited for thermoplastic-based composites such as PEEK/HA, enabling the construction of porous architectures with tunable mechanical properties tailored for load-bearing applications.122 DIW has been employed to fabricate the Ti/β-TCP scaffolds for bone reconstruction, exhibiting satisfactory biomechanical and biological properties.123 Multi-material jetting further expand capabilities by allowing simultaneous deposition of polymers and ceramic, producing multi-materials ceramic parts with high precision, good interfacial bonding and no defects.68 However, the application of composite biomaterials in AM-fabricated CMFIs remains limited, with relatively few studies reported to date. This is primarily due to challenges in material compatibility and process control. Differences in thermal and rheological properties among composite constituents’ complicate fabrication, while extrusion- and powder-based AM techniques often suffer from narrow processing windows and poor reproducibility.124 Table 3 summarizes representative clinical cases of CMFIs fabricated using various AM technologies over the past five years.
Surface morphology and post-processing
Surface morphology and roughness play a crucial role in the biological performance of additively manufactured implants, influencing early-stage cell adhesion, bacterial colonization, and the generation of wear particles. For example, unprocessed FFF-printed PEEK exhibits a high surface roughness (Ra ~22.28 μm), which can promote osteoblast attachment and growth. Likewise, SLM and EBM typically produce relatively rough surfaces (Ra ~5–20 μm) that support osteoblast adhesion but may also increase the risk of bacterial biofilm formation—particularly in mandibular implants exposed to the oral microbiome.125 In contrast, DLP yields significantly smoother surfaces, which are favorable for minimizing neural tissue irritation in cranial applications.126 Mechanical surface modifications such as polishing and sandblasting are commonly employed to reduce roughness and improve tissue integration.
A variety of advanced post-processing strategies have been developed to further enhance implant functionality. Electropolishing and plasma polishing can reduce surface roughness by up to 40% and 30% in SLM- and EBM-fabricated implants, respectively, improving both biocompatibility and fatigue resistance.127 Ultrasonic cleaning has proven effective in removing up to 95% of residual powder from complex lattice structures such as gyroids, thereby mitigating the risk of chronic inflammation or foreign body response.128 Additionally, femtosecond and picosecond laser treatments have emerged as precise methods for creating micro- and nanoscale textures on titanium alloy surfaces, enhancing osteoblast proliferation while reducing bacterial adhesion through modified surface chemistry. Electrochemical deposition of HA coatings—especially those with nanoplates—has also been shown to significantly improve protein adsorption, osteogenic differentiation, and stromal cell proliferation, offering an effective route to biofunctionalized metallic implants.129
The integration of these surface modification techniques into the fabrication of AM implants holds significant promise for advancing implant performance. By tailoring surface characteristics at the micro and nanoscale, it is possible to achieve a synergistic enhancement of biological compatibility and mechanical robustness,130 paving the way for next-generation CMFIs. Nonetheless, extensive post-processing poses its own challenges. Aggressive surface modification or internal cleaning may inadvertently alter critical pore geometries or reduce structural integrity, particularly in thin-walled or highly porous regions.131,132 Therefore, there is a pressing need for standardized, material-specific and geometry-specific post-processing protocols that preserve geometric fidelity.133,134
Challenges in maintaining the “3Bs” in AM
The dimensional accuracy of AM plays a critical role in determining the “3Bs” performance of CMFIs. Deviations from the intended design—resulting from powder adhesion, thermal distortion, or incomplete removal of support structures—can significantly alter pore size, interconnectivity, and overall porosity, thereby impairing osteoconduction, mechanical stability, and osseointegration.135 SLM typically achieves dimensional tolerances within ±50 μm, which is generally adequate for mandibular reconstructions requiring mechanical robustness and anatomical conformity. In contrast, electron beam melting (EBM) exhibits slightly lower resolution (±100 μm), necessitating tighter control when used for cranial implants where thin cortical structures and curvature demand higher geometric fidelity.136 The results of DIW-based implants showed an overall unsigned dimensional deviation of (30.1 ± 20.2) μm, with a median of 24.4 μm, indicating adequate precision for CMFIs applications.137 DLP offers superior accuracy (±20 μm), making it well-suited for intricate craniofacial scaffolds with fine anatomical details.138
In addition to dimensional accuracy, each AM techniques exhibit inherent limitations. Metal AM processes typically require extensive post-processing steps—such as stress-relief annealing, precision machining, and surface finishing—to mitigate residual stresses and achieve the desired surface quality.139 In polymer-based AM, the layer-by-layer deposition approach often results in anisotropic mechanical properties, primarily due to weaker interlayer bonding compared to the bulk material.140 This anisotropy can significantly compromise load-bearing capacity and long-term mechanical durability, particularly in anatomically complex and mechanically demanding applications such as mandibular reconstruction. Bioceramic materials are intrinsically brittle, which constrains the geometric complexity and mechanical robustness of the printed constructs.141 Moreover, shrinkage and warping during the drying and sintering stages may lead to the formation of internal defects such as cracks or voids. Achieving adequate mechanical strength in highly porous bioceramics structures remains a significant challenge, especially for load-bearing applications. Additionally, common AM-induced defects—such as voids, incomplete fusion, and irregular microstructures—can serve as stress concentrators, ultimately reducing the structural integrity and reliability of the final implants.142
Preclinical evaluation
To date, there is no end-to-end platform capable of comprehensively evaluating CMFIs across the “3Bs” scales. However, a wide range of mature and emerging methodologies exist for assessing performance within each individual dimension. For instance, biomechanical evaluation can be conducted using finite element analysis and mechanical testing platforms; biocompatibility is commonly assessed through in vitro cell culture and in vivo animal injection models; while bioactivity is often evaluated using techniques such as bone fluorescent labeling and computed tomography imaging (Fig. 3). This section focuses on well-established and widely adopted evaluation methods, laying the groundwork for integrating mainstream assessment techniques into a unified, large-scale development platform in the future.

Overview of common preclinical assessment methodologies for CMFIs
Biomechanical assessment
Biomechanical investigations of CMFIs have primarily addressed four aspects: (1) Mechanical strength, including compressive, bending, and torsional properties, which are critical for ensuring the structural integrity and biomechanical stability of implants. (2) Stress shielding, which addresses the need for continuous and physiologically appropriate stress distribution to promote bone regeneration. Studies have demonstrated that the porous titanium mesh induced less stress shielding compared to the dense titanium plate.104 (3) Fatigue behavior, which is particularly significant for mandibular and orbital implants subjected to cyclic loading due to masticatory and facial movements. Research highlights that variable amplitude loading can dramatically affect crack growth in the PMMA implants.143 (4) Fixation methods, which influence the mechanical stability of the implant-bone interface. For example, comparative analyses suggest that “wing”-type fixation methods produce lower stress concentrations than alternative approaches.144 Biomechanical analysis techniques employed in CMFI research can be broadly categorized into experimental mechanics and computational simulations.
For experimental mechanics, tensile and compressive tests on CMFIs are typically conducted using a universal testing machine. Bending tests, such as three-point or four-point bending, evaluate flexural properties. Shear tests assess a material’s resistance to sliding forces, often applied to composites and joints.51 Additionally, dynamic mechanical analysis (DMA) and fatigue testing machines are employed to study materials under cyclic loading and time-dependent behavior. Advanced techniques such as Digital Image Correlation (DIC) and micro-Computed Tomography (micro-CT) are increasingly integrated into mechanical experiments.145 DIC enables full-field strain measurement by tracking surface deformations in real time, enhancing the understanding of local mechanical responses. Micro-CT provides high-resolution 3D imaging of internal structures, allowing non-destructive evaluation of damage evolution. However, despite their utility, experimental mechanical tests often fall short of replicating the physiological complexity encountered in vivo. Static loading tests do not account for fatigue damage accumulation over time, and fatigue tests with constant amplitude cycles may not adequately represent the variable loading conditions of daily activities.
The Finite Element Method (FEM), a widely recognized numerical approach for mechanical simulations, has long been employed to predict the mechanical behavior of implants under complex loading conditions (e.g., mandible reconstruction), which are often challenging to replicate in experimental setups.146 However, FEM typically overlooks the synergistic interactions with biological factors, such as bone-implant integration, tissue ingrowth, and the evolution of mechanical properties during the healing process. Realistic modeling of these interactions necessitates complex multi-scale or growth-adaptive simulations, which, while promising, remain computationally demanding. Thus, recent studies have proposed novel numerical methods to address these challenges. For instance, the integration of musculoskeletal multibody dynamics (MSK-MBD) with FEM has enabled the consideration of muscle and temporomandibular joint (TMJ) influences in the craniomaxillofacial region.147,148 Additionally, the combination of machine learning (ML) and FEM has proven effective in reducing computational costs, thus enhancing the efficiency of biomechanical simulations.149 However, the accuracy of simulation models still requires comprehensive validations to enable accurate predictions in complex craniomaxillofacial environments.
Biocompatibility assessment
Ensuring that CMFIs are non-toxic, non-immunogenic, and clinically safe has been the central aim of biocompatibility studies. Standard in vitro evaluation methods include cytotoxicity assays (e.g., MTT, CCK-8), as well as assessments of cell adhesion, proliferation, and inflammatory responses through cytokine profiling.150 Recent advanced models such as three-dimensional (3D) co-culture systems, organoid models, and organ-on-a-chip platforms have emerged, providing a more physiologically relevant context by recapitulating cell–cell interactions and tissue architecture. In addition, transcriptomic and proteomic analyses offer molecular-level insights into cellular responses to biomaterials, thereby deepening our understanding of biocompatibility mechanisms. Immune-related in vitro assays, particularly those assessing macrophage polarization (M1/M2), are increasingly employed to evaluate the immunomodulatory properties of candidate materials.151 Real-time cell analysis (RTCA) as a dynamic, label-free technique for continuously monitoring cell behavior on biomaterials. This method is particularly advantageous for evaluating biodegradable materials, providing real-time data on cell adhesion and proliferation dynamics.152
In vivo biocompatibility assessments involve subcutaneous or intramuscular implantation of materials into animal models to evaluate tissue responses such as inflammation, fibrosis, and immune activation. Histological analysis and systemic immune profiling are commonly employed to assess local and systemic biocompatibility. Critical-sized bone defects are surgically created in the calvarial, mandibular, or orbital regions of animals (typically rats, rabbits, dogs, or sheep) to simulate clinically relevant craniofacial injuries.153 Defect sizes vary by species (e.g., 5–8 mm in rats, 8–15 mm in rabbits),154 and CMFIs are implanted and monitored over periods ranging from weeks to months. Additionally, multi-omics profiling and single-cell sequencing are being integrated into in vivo studies to dissect the cellular heterogeneity and molecular crosstalk involved in scaffold-mediated bone regeneration.155 These approaches provide deeper insight into the mechanisms of immune-bone crosstalk, especially the roles of macrophage polarization, T-cell subsets, and the osteo immunomodulatory environment.
However, several limitations continue to constrain clinical translation. While in vitro assays are indispensable for early screening, they fail to recapitulate the dynamic mechanical loadings, immunologically active, and vascularized environment of living bone.156,157 Moreover, most in vivo studies are limited to short-term or medium-term evaluation (typically ≤12 weeks), leaving critical questions about long-term degradation, chronic inflammation, and implant integration unresolved.158 The absence of standardized protocols across laboratories—especially regarding defect models, cell types, culture durations, and outcome measures—further complicates comparison and slows clinical translation.159
Bioactivity assessment
Bioactivity evaluations, in contrast, focus on the capacity of implants to actively promote bone regeneration and vascularization. Osteoblast-like cells (e.g., MC3T3-E1 pre-osteoblasts, human mesenchymal stem cells) are typically seeded onto material surfaces or scaffolds to evaluate cellular attachment, viability, and differentiation.160 Common assays include viability staining (e.g., MTT, XTT), ALP activity assays, mineralization analysis via Alizarin Red staining,160 and the expression of osteogenic markers such as Runx2 and OCN.161 Angiogenic potential is evaluated through endothelial cell assays, including tube formation and VEGF expression.162 Recently, three-dimensional co-culture models combining osteoblasts and endothelial cells have been developed to better simulate the osteoangiogenic microenvironment and provide more physiologically relevant insights into the bioactivity of scaffolds.163 In addition, microfluidic systems and organ-on-a-chip technologies are being explored to replicate the dynamic interplay between bone and vasculature under controlled flow conditions.164 These platforms allow for real-time monitoring of cellular behavior and facilitate high-content analysis of biomaterial-induced responses.
In vivo bone regeneration is commonly studied using critical-sized defect models in craniomaxillofacial bones (e.g., calvarial, mandibular, orbital) of rats, rabbits, dogs, or sheep to mimic human clinical conditions.165 Genetically modified or immunodeficient animals are increasingly employed to evaluate human cell-based constructs or dissect specific molecular mechanisms. The in vivo bioreactor (IVB) approach, which leverages the body’s intrinsic regenerative capacity through flap prefabrication and axial vascularization, represents a promising direction for personalized bone tissue engineering. Its efficacy has been demonstrated in multiple preclinical models.166 Bone healing has been evaluated through histological staining and immunohistochemistry using markers such as osteocalcin (OCN) and CD31.167,168 More recently, in silico approaches have been integrated with in vivo animal models to enhance the assessment of bone regeneration. For example, non-invasive imaging modalities—including micro-computed tomography (micro-CT, e.g., bone volume to total volume ratio [BV/TV] analysis), magnetic resonance imaging (MRI), and positron emission tomography-computed tomography (PET-CT)—enable dynamic monitoring of bone formation, scaffold degradation, and host tissue integration.169
However, existing methodologies for assessing bioactivity are subject to several inherent challenges. In vitro models, though essential for early-stage screening, often oversimplify the complex osteoimmune and angiogenic environments found in vivo. Traditional 2D cultures fail to replicate the three-dimensional architecture and dynamic cell–matrix interactions critical to bone regeneration.170 In vivo animal models, while more physiologically relevant, come with their own constraints. Standard markers such as ALP activity and mineral deposition do not capture the effects of mechanical loading, immune modulation, or nutrient diffusion that influence long-term osseointegration.171 Small animals such as rats or rabbits have faster bone regeneration rates and different bone turnover dynamics compared to humans, potentially leading to overestimation of regenerative efficacy.172,173,174
Next-generation CMFIs
Given the current limitations in biomaterials, design architectures, AM technologies, and preclinical evaluation methods, breakthroughs at multiple levels are urgently needed to develop next-generation CMFIs that achieve balanced and satisfactory performance within the “3Bs” evaluation framework. This review proposes four key directions for future breakthroughs in next-generation CMFIs: (1) Smart and 4D-printing biomaterials; (2) AI-driven design optimization; (3) Predictable models for additive manufacturing; (4) Next-generation platforms for preclinical design and evaluation.
Smart and 4D-printing biomaterials
To date, no single biomaterial has proven capable of fully balancing biomechanics, biocompatibility, and bioactivity. Clinical decision-making requires careful trade-offs. For example, titanium offers high compatibility and stability but severe stress shielding; PEEK offers desired biomechanical performance but is inert. Thus, the development of biomaterials for CMFIs has evolved from the use of single-component materials to composites with nanoparticles. These biomaterials aim to hit the “sweet spot” by combining materials that together meet multiple criteria. For example, titanium meshes was combined with bioactive coatings or bioroot substitutes.175 PEEK could be surface-modified or loaded with bioactive particles.46 3D-printed implants with a stiff titanium frame surrounded by a softer, porous polymer-ceramic composite layer. This graded stiffness mimics the transition from cortical bone to marrow or soft tissue. Another concept is an implant with an embedded bioresorbable core and a permanent outer shell. The core provides initial strength and then disappears as bone regenerates.176 Fig. 4 shows the development of the biomaterials for CMFIs in recent years.

Biomaterials roadmap of CMFIs: from traditional biomaterials to future biomaterials
Recent reviews note that integrating smart materials (e.g., shape-memory polymers (SMPs), magnetically responsive composites) into 3D printed constructs could yield dynamic implants that adapt mechanically or deliver drugs on demand, which is also known as 4D printing biomaterials. 4D printing represents the convergence of additive manufacturing and smart materials, enabling the fabrication of time-dependent, stimulus-responsive implants tailored to dynamic biological environments.177 For instance, a compressed Ni-Ti mesh might expand once heated to body temperature, securing itself in a bone bed without extensive screws and enabling minimally invasive implantation.178 A folded SMPs-based implants could expand in situ to fit a bone defect.179 Future implants may also include bioelectronics (thin-film biosensors) to monitor pressure or strain at the implant–bone interface in real time, alerting clinicians to complications before clinical symptoms appear.180 Smart piezoelectric materials scaffolds has also been reported to promote cell proliferation and regeneration of damaged tissues.181 Although most of these smart materials remain at the conceptual stage, their integration is anticipated to represent a future trend in the development of CMFIs which comprehensively balance the “3Bs” performance.
AI-driven design optimization
Design optimization plays a pivotal role in enhancing the “3Bs” performance of CMFIs. However, the extensive design freedom of CMFIs—including variations in materials, geometry, and internal architecture—demands substantial computational resources. Moreover, the design process often demands substantial time investment in CAD modeling and computational simulation, which poses a challenge for timely clinical translation in urgent scenarios. Artificial intelligence (AI) has transformed computational design optimization by enabling efficient exploration of complex, high-dimensional design spaces, by reducing dependence on time-consuming simulations and experimental iterations.182,183 The integration of AI to predict and harmonize 3Bs performance presents a transformative strategy for the development of next-generation CMFIs.
Recent efforts have explored the application of AI in the design optimization of CMFIs. Machine learning models, such as convolutional neural networks (CNNs), predict stress distribution, fatigue life, and osseointegration based on TPMS geometry and material inputs of the implants. For examples, a ML model predicted fatigue life of TPMS-based femoral scaffolds with 95% accuracy, minimizing the need for extensive mechanical testing.101 Another study uses a machine learning–based model to quickly predict how different factors affect bone growth on 3D-printed biodegradable bone scaffolds. It identifies optimal material and loading conditions to improve bone cell formation, helping to speed up scaffold design.184 Additionally, a study demonstrates the potential of AI-optimized Gyroid lattice scaffolds, designed with advanced composites, to enhance mechanical performance and biocompatibility for personalized orthopedic implants.185 Although not directly targeting CMFIs, these studies introduce the concept of AI-driven design iteration, enabling real-time, patient-specific design optimization with minimal human intervention and improved implant performance across anatomical sites. Furthermore, leveraging the end-to-end platform presented in Section 6.4, CMFIs design data can be shared among the users, potentially accumulating more data to train the AI model to enable more efficient and accurate AI-driven design optimization.
Predictable models for additive manufacturing
Although AM technology has revolutionized the fabrication of CMFIs—enabling patient-specific geometries, controlled porosity, and on-demand material deposition—a clear gap remains between the theoretical design models and the actual performance of printed structures.186 Variations introduced during printing—such as thermal gradients, microstructural inhomogeneities, surface roughness, and printing resolution limits—can significantly alter the “3Bs” behavior of the final implant.187 As a result, many CMFIs based on digital design fail to achieve their intended function in vivo. Consequently, it is a future direction to predict inherent deviations induced by the AM process, and to accordingly adjust the biomaterial selection and design architectures of CMFIs during the pre-design stage, in order to ensure that the manufactured implants achieve the intended performance among the “3Bs”.
To address this, next-generation CMFIs must incorporate process-aware modeling frameworks that explicitly account for the manufacturing process parameters—such as energy input, layer height, scanning speed, and sintering behavior—into performance predictions. For instance, integrated AM–FEM workflows, where printing-induced defects, residual stresses, or local porosity are captured and fed into mechanical or biological simulations, could drastically improve predictive accuracy.188,189,190 In parallel, machine learning models trained on experimental and computational datasets linking AM parameters to final part performance (e.g., compressive strength, degradation rate, bioactivity) offer a promising route to inverse design—where target properties can be used to suggest optimal printing parameters.191,192,193 Additionally, real-time in situ monitoring and imaging techniques (e.g., optical tomography, micro-CT) can provide feedback loops to calibrate and validate predictive models.194 Ultimately, bridging the gap between design intent and manufacturing reality will require a convergence of material science, manufacturing process control, and multiscale modeling. This integration will not only improve the reliability and reproducibility of AM implants but also enable true “print-and-predict” capabilities for next-generation CMFIs and patient-specific bone reconstruction.
Multiscale preclinical design and evaluation platform
Despite significant progress in the development of biomaterials, design architectures and AM technology, current preclinical platforms remain limited in their ability to fully capture the complexity of bone biomechanics (e.g., temporomandibular joint dynamics), patient-specific anatomy, long-term biocompatibility and implant osseointegrations.195 Moreover, the current development process of CMFIs typically relies on multiple independent platforms, each utilizing distinct data formats. The interfaces between these steps are often complex and time-consuming. For instance, 3D reconstruction data must be sequentially processed by CAD software, numerical simulation tools, and optimization algorithms. Although certain commercial solutions, such as Materialise, have made substantial efforts to integrate these functions into a unified platform, they still fall short of supporting a fully streamlined design and evaluation workflow. Therefore, next-generation preclinical design and evaluation platform for CMFIs is expected to evolve toward advanced, integrated, multiscale, AI-enhanced, and data-driven frameworks (Fig. 5).

Conceptual diagram of future preclinical design and evaluation platform. CAD computer-aided design, CAE computer-aided engineering, CAM computer-aided manufacturing
This future platform provides a scalable foundation for the integration of the emerging and high-impact technologies. For example, digital twin will enable real-time, personalized predictions of implant performance, creating a virtual replica of the implant-bone system based on patient-specific imaging, biomechanical data, and biological responses.196 A digital twin of a mandibular reconstruction implant can continuously simulate bone ingrowth and stress distribution under masticatory loads, providing early warnings of mechanical failure or poor osseointegration.197 Meanwhile, high-throughput experimental platforms, such as automated bioreactor arrays and image-based screening systems, will accelerate in vitro evaluation of materials, topographies, and biological responses.198 The convergence of in vivo, in vitro, and in silico approaches will form a closed-loop pipeline, in which computational predictions are validated experimentally and iteratively refined. Furthermore, an emerging bio-chemo-mechanical multiscale model could be used to simultaneously monitor “3Bs” behavior of the implants.199 To summarize, this future design and evaluation platform is anticipated to significantly shorten development cycles and improve the safety, efficacy, and individualization of next-generation CMFIs.
Limitations and challenges for clinical translation of next-generation CMFIs
While Sections “Smart and 4D-Printing Biomaterials”–“Multiscale Preclinical Design and Evaluation Platform” outlined the emerging materials, technologies and platforms that underpin next-generation CMFIs, their translation into clinical practice faces several key challenges. First, regulatory hurdles remain a major bottleneck, particularly for multi-material, 4D-printed, and stimulus-responsive implants, which introduce additional complexity in safety validation, long-term reliability, and risk assessment.200 Second, economic and scalability constraints limit widespread adoption. Advanced AM processes, digital twin platforms, and AI-driven design optimization require substantial computational resources, specialized equipment, and expert personnel, making cost-effectiveness and large-scale implementation challenging.182 Third, experimental validation and evidence gaps persist: predictive AM models and AI-optimized designs, while highly promising, rely on limited laboratory-scale or small-animal studies, with scarce large-animal or clinical data to confirm safety, efficacy, and generalizability.201 Addressing these limitations—including regulatory, economic, and validation-related challenges—will be essential to bridge the gap between experimental innovations and reliable clinical applications of next-generation CMFIs.
Conclusion
Next-generation CMFIs represent a transformative frontier in personalized craniomaxillofacial bone reconstruction, aiming to optimize the interplay among biomechanics, biocompatibility, and bioactivity—the “3Bs”. This review outlines the current advances in material innovations, design strategies, additive manufacturing, and preclinical evaluation methodologies that collectively drive this evolution. Emerging biomaterials, including bioresorbable polymers, magnesium alloys, bioactive ceramics, and composites with nanoparticles expand the possibilities for patient-specific solutions. Innovative designs, such as TPMS architectures, offer unprecedented control over mechanical properties and biological responses. Additive manufacturing enables the creation of geometrically complex, functional implants tailored to individual anatomical and pathological needs. Concurrently, preclinical evaluation frameworks—spanning multiscale biomechanical testing, biological assays, and in vivo animal models—provide critical insight into the performance of CMFIs.
Looking forward, several frontiers will shape the future of CMFIs development:
-
Smart and 4D-printing biomaterials will empower implants to dynamically adapt to the evolving biological environment.
-
AI-driven design optimization frameworks will enable data-informed optimization across structural and biological domains.
-
Predictive models for additive manufacturing will ensure reproducibility, precision, and customization in CMFIs fabrication.
-
Multiscale preclinical design and evaluation platforms, integrating advanced multiscale assessing model and AI-enhanced systems, will offer more accurate and reliable evaluation tools, bridging the gap between benchtop and bedside.
Ultimately, a translational pipeline integrating cutting-edge biomaterials science, AI-assisted design, predictive fabrication, and rigorous evaluation will be essential to bring next-generation CMFIs from concept to clinical success. Interdisciplinary collaboration across biomedical engineering, materials science, computational modeling, and clinical practice will be key to realizing the full potential of this promising field.
References
-
Jaiswal, R. & Pu, L. L. Q. Reconstruction after complex facial trauma: Achieving optimal outcome through multiple contemporary surgeries. Ann. Plast. Surg. 70, 406–409 (2013).
-
Crist, T. E., Mathew, P. J., Plotsker, E. L., Sevilla, A. C. & Thaller, S. R. Biomaterials in craniomaxillofacial reconstruction: Past, present, and future. J. Craniofacial Surg. 32, 535–540 (2021).
-
Chen, W. et al. Craniofacial resection and reconstruction in patients with recurrent cancer involving the craniomaxillofacial region. J. Oral. Maxillofac. Surg. 75, 622–631 (2017).
-
Posch, N. A. S., Mureau, M. A. M., Dumans, A. G. & Hofer, S. O. P. Functional and aesthetic outcome and survival after double free flap reconstruction in advanced head and neck cancer patients. Plast. Reconstructive Surg. 120, 124–129 (2007).
-
Hofer, S. & Payne, C. Functional and aesthetic outcome enhancement of head and neck reconstruction through secondary procedures. Semin. Plast. Surg. 24, 309–318 (2010).
-
Wang, W. & Yeung, K. W. K. Bone grafts and biomaterials substitutes for bone defect repair: A review. Bioact. Mater. 2, 224–247 (2017).
-
LaPrade, R. F. & Botker, J. C. Donor-site morbidity after osteochondral autograft transfer procedures. Arthrosc.: J. Arthroscopic Relat. Surg. 20, e69–e73 (2004).
-
Graham, S. M. et al. Biological therapy of bone defects: the immunology of bone allo-transplantation. Expert Opin. Biol. Ther. 10, 885–901 (2010).
-
Boneva, R. S., Folks, T. M. & Chapman, L. E. Infectious Disease Issues in Xenotransplantation. Clin. Microbiol Rev. 14, 1–14 (2001).
-
Thayaparan, G. K., Lewis, P. M., Thompson, R. G. & D’Urso, P. S. Patient-specific implants for craniomaxillofacial surgery: A manufacturer’s experience. Ann. Med. Surg. 66, 102420 (2021).
-
Dewey, M. J. & Harley, B. A. C. Biomaterial design strategies to address obstacles in craniomaxillofacial bone repair. RSC Adv. 11, 17809–17827 (2021).
-
Gupta, S., Gupta, H. & Tandan, A. Technical complications of implant-causes and management: A comprehensive review. Natl. J. Maxillofac. Surg. 6, 3 (2015).
-
Tabrizian, P., Davis, S. & Su, B. From bone to nacre – development of biomimetic materials for bone implants: a review. Biomater. Sci. 12, 5680–5703 (2024).
-
Selim, M., Mousa, H. M., Abdel-Jaber, G. T., Barhoum, A. & Abdal-hay, A. Innovative designs of 3D scaffolds for bone tissue regeneration: Understanding principles and addressing challenges. Eur. Polym. J. 215, 113251 (2024).
-
Koppunur, R. et al. Design and fabrication of patient-specific implant for maxillofacial surgery using additive manufacturing. Adv. Mater. Sci. Eng. 2022, 1–7 (2022).
-
Shaikh, M. et al. Revolutionising orthopaedic implants—a comprehensive review on metal 3D printing with materials, design strategies, manufacturing technologies, and post-process machining advancements. Int. J. Adv. Manuf. Technol. 134, 1043–1076 (2024).
-
Hériveaux, Y. et al. Mechanical micromodeling of stress-shielding at the bone-implant interphase under shear loading. Med Biol. Eng. Comput 60, 3281–3293 (2022).
-
Naujokat, H. et al. In vivo biocompatibility evaluation of 3D-printed nickel–titanium fabricated by selective laser melting. J. Mater. Sci. Mater. Med. 33, 13 (2022).
-
Al Maruf, D. S. A. et al. Evaluation of osseointegration of plasma treated polyaryletherketone maxillofacial implants. Sci. Rep. 15, 1895 (2025).
-
Figueroa-Sanchez, J. A. et al. Partial cranial reconstruction using titanium mesh after craniectomy: An antiadhesive and protective barrier with improved aesthetic outcomes. World Neurosurg. 185, 207–215 (2024).
-
Wong, R. C. W., Tideman, H., Merkx, M. A. W., Jansen, J. & Goh, S. M. The modular endoprosthesis for mandibular body replacement. Part 1: Mechanical testing of the reconstruction. J. Cranio-Maxillofac. Surg. 40, e479–e486 (2012).
-
Pakdel, A. R., Whyne, C. M. & Fialkov, J. A. Structural biomechanics of the craniomaxillofacial skeleton under maximal masticatory loading: Inferences and critical analysis based on a validated computational model. J. Plast., Reconstr. Aesthet. Surg. 70, 842–850 (2017).
-
Lang, J. J. et al. Improving mandibular reconstruction by using topology optimization, patient specific design and additive manufacturing?—A biomechanical comparison against miniplates on human specimen. PLoS ONE 16, e0253002 (2021).
-
Rosa, V. et al. Guidance on the assessment of biocompatibility of biomaterials: Fundamentals and testing considerations. Dent. Mater. 40, 1773–1785 (2024).
-
Huzum, B. et al. Biocompatibility assessment of biomaterials used in orthopedic devices: An overview (Review). Exp. Ther. Med. 22, 1315 (2021).
-
Pappalardo, D., Mathisen, T. & Finne-Wistrand, A. Biocompatibility of resorbable polymers: A historical perspective and framework for the future. Biomacromolecules 20, 1465–1477 (2019).
-
Szwed-Georgiou, A. et al. Bioactive materials for bone regeneration: Biomolecules and delivery systems. ACS Biomater. Sci. Eng. 9, 5222–5254 (2023).
-
Zhao, B. et al. Promoting osteoblast proliferation on polymer bone substitutes with bone-like structure by combining hydroxyapatite and bioactive glass. Mater. Sci. Eng.: C. 96, 1–9 (2019).
-
Lim, H.-K., Choi, Y.-J., Choi, W.-C., Song, I.-S. & Lee, U.-L. Reconstruction of maxillofacial bone defects using patient-specific long-lasting titanium implants. Sci. Rep. 12, 7538 (2022).
-
Shaikh, M. Q. et al. Investigation of patient-specific maxillofacial implant prototype development by metal fused filament fabrication (MF3) of Ti-6Al-4V. Dent. J. 9, 109 (2021).
-
Brogini, S. et al. In vivo validation of highly customized cranial Ti-6AL-4V ELI prostheses fabricated through incremental forming and superplastic forming: an ovine model study. Sci. Rep. 14, 7959 (2024).
-
Hijazi, K. M., Dixon, S. J., Armstrong, J. E. & Rizkalla, A. S. Titanium alloy implants with lattice structures for mandibular reconstruction. Materials 17, 140 (2023).
-
Bittredge, O. et al. Fabrication and optimisation of Ti-6Al-4V lattice-structured total shoulder implants using laser additive manufacturing. Materials 15, 3095 (2022).
-
Villapun Puzas, V. M. et al. Surface free energy dominates the biological interactions of postprocessed additively manufactured Ti-6Al-4V. ACS Biomater. Sci. Eng. 8, 4311–4326 (2022).
-
Park, J.-H. et al. 3D-printed titanium implant with pre-mounted dental implants for mandible reconstruction: a case report. Maxillofac. Plast. Reconstr. Surg. 42, 28 (2020).
-
Ardila, C.-M., Hernández-Arenas, Y. & Álvarez-Martínez, E. Mandibular body reconstruction utilizing a three-dimensional custom-made porous titanium plate: A four-year follow-up clinical report. Case Rep. Dent. 2022, 5702066 (2022).
-
Liu, R. et al. Novel design and optimization of porous titanium structure for mandibular reconstruction. Appl. Bionics Biomech. 2022, 1–13 (2022).
-
Li, H., Hao, J. & Liu, X. Research progress and perspective of metallic implant biomaterials for craniomaxillofacial surgeries. Biomater. Sci. 12, 252–269 (2024).
-
Xue, R. et al. Finite element analysis and clinical application of 3D-printed Ti alloy implant for the reconstruction of mandibular defects. BMC Oral. Health 24, 95 (2024).
-
Sunderland, I. R., Edwards, G., Mainprize, J. & Antonyshyn, O. A technique for intraoperative creation of patient-specific titanium mesh implants. Plast. Surg. 23, 95–99 (2015).
-
Gareb, B., Van Bakelen, N. B., Vissink, A., Bos, R. R. M. & Van Minnen, B. Titanium or biodegradable osteosynthesis in maxillofacial surgery? in vitro and in vivo performances. Polymers 14, 2782 (2022).
-
Vujović, S. et al. Applications of biodegradable magnesium-based materials in reconstructive oral and maxillofacial surgery: A review. Molecules 27, 5529 (2022).
-
Prasadh, S. et al. The potential of magnesium based materials in mandibular reconstruction. Metals 9, 302 (2019).
-
Gugliotta, Y., Zavattero, E., Ramieri, G., Borbon, C. & Gerbino, G. Cranio-Maxillo-facial reconstruction with polyetheretherketone patient-specific implants: Aesthetic and functional outcomes. JPM 14, 849 (2024).
-
Anderson, B. et al. Comparison of perioperative and long-term outcomes following PEEK and autologous cranioplasty: A single institution experience and review of the literature. World Neurosurg. 180, e127–e134 (2023).
-
Kauke-Navarro, M., Knoedler, L., Knoedler, S., Deniz, C. & Safi, A.-F. Surface modification of PEEK implants for craniofacial reconstruction and aesthetic augmentation—fiction or reality?. Front. Surg. 11, 1351749 (2024).
-
Cárdenas-Serres, C. et al. Custom CAD/CAM peek implants for complex orbitocranial reconstruction: Our experience with 15 patients. JCM 13, 695 (2024).
-
Punchak, M. et al. Outcomes following polyetheretherketone (PEEK) cranioplasty: Systematic review and meta-analysis. J. Clin. Neurosci. 41, 30–35 (2017).
-
Verma, S., Sharma, N., Kango, S. & Sharma, S. Developments of PEEK (Polyetheretherketone) as a biomedical material: A focused review. Eur. Polym. J. 147, 110295 (2021).
-
Bello-Rojas, G., Whitney, M., Rontal, M. & Jackson, I. T. Long-term results of craniofacial implantation: a return to methyl methacrylate. Eur. J. Plast. Surg. 35, 177–180 (2012).
-
Msallem, B. et al. Biomechanical evaluation of patient-specific polymethylmethacrylate cranial implants for virtual surgical planning: An in-vitro study. Materials 15, 1970 (2022).
-
Huang, G. J. et al. Craniofacial reconstruction with poly(methyl methacrylate) customized cranial implants. J. Craniofacial Surg. 26, 64–70 (2015).
-
Prasadh, S. & Wong, R. C. W. Unraveling the mechanical strength of biomaterials used as a bone scaffold in oral and maxillofacial defects. Oral. Sci. Int. 15, 48–55 (2018).
-
Dwivedi, R. et al. Polycaprolactone as biomaterial for bone scaffolds: Review of literature. J. Oral. Biol. Craniofacial Res. 10, 381–388 (2020).
-
Martini, L. et al. Long-term results following cranial hydroxyapatite prosthesis implantation in a large skull defect model. Plast. Reconstr. Surg. 129, 625e–635e (2012).
-
De Carvalho, A. B. G. et al. Personalized bioceramic grafts for craniomaxillofacial bone regeneration. Int J. Oral. Sci. 16, 62 (2024).
-
Elemosho, A., Kluemper, J. C., Pfahl, E. & Mitchell, K.-A. S. Outcomes of hydroxyapatite bone cement for craniofacial reconstruction in 1983 patients. J. Craniofacial Surg. 36, 115–118 (2025).
-
Systermans, S. et al. An innovative 3D hydroxyapatite patient-specific implant for maxillofacial bone reconstruction: A case series of 13 patients. J. Cranio-Maxillofac. Surg. 52, 420–431 (2024).
-
Shen, C. et al. Transforming the degradation rate of β-tricalcium phosphate bone replacement using 3-dimensional printing. Ann. Plast. Surg. 87, e153–e162 (2021).
-
Houmard, M., Fu, Q., Genet, M., Saiz, E. & Tomsia, A. P. On the structural, mechanical, and biodegradation properties of HA/β-TCP robocast scaffolds: Bone-substitute material in various tissue-engineering applications. J. Biomed. Mater. Res 101, 1233–1242 (2013).
-
Chen, Q. Z., Thompson, I. D. & Boccaccini, A. R. 45S5 Bioglass®-derived glass–ceramic scaffolds for bone tissue engineering. Biomaterials 27, 2414–2425 (2006).
-
Kaur, G. et al. Mechanical properties of bioactive glasses, ceramics, glass-ceramics and composites: State-of-the-art review and future challenges. Mater. Sci. Eng.: C. 104, 109895 (2019).
-
Shekhawat, D., Singh, A., Banerjee, M. K., Singh, T. & Patnaik, A. Bioceramic composites for orthopaedic applications: A comprehensive review of mechanical, biological, and microstructural properties. Ceram. Int. 47, 3013–3030 (2021).
-
Ma, R. & Guo, D. Evaluating the bioactivity of a hydroxyapatite-incorporated polyetheretherketone biocomposite. J. Orthop. Surg. Res 14, 32 (2019).
-
Zheng, J. et al. Additively-manufactured PEEK/HA porous scaffolds with highly-controllable mechanical properties and excellent biocompatibility. Mater. Sci. Eng.: C. 128, 112333 (2021).
-
Osawa, S., Hashikawa, K., Naruse, H. & Terashi, H. Clinical evaluation of unsintered hydroxyapatite particles/poly L-lactide composite device in craniofacial surgery. J. Craniofacial Surg. 32, 2148–2151 (2021).
-
Ramanathan, M. et al. In vivo evaluation of bone regenerative capacity of the novel nanobiomaterial: β-tricalcium phosphate polylactic acid-co-glycolide (β-TCP/PLLA/PGA) for use in maxillofacial bone defects. Nanomaterials 14, 91 (2023).
-
Sun, H. et al. Multi-material ceramic hybrid additive manufacturing based on vat photopolymerization and material extrusion compound process. Addit. Manuf. 97, 104627 (2025).
-
Saikia, N. Inorganic-based nanoparticles and biomaterials as biocompatible scaffolds for regenerative medicine and tissue engineering: Current advances and trends of development. Inorganics 12, 292 (2024).
-
Trzaskowska, M. et al. Biocompatible nanocomposite hydroxyapatite-based granules with increased specific surface area and bioresorbability for bone regenerative medicine applications. Sci. Rep. 14, 28137 (2024).
-
Cazan, C., Enesca, A. & Andronic, L. Synergic effect of TiO2 filler on the mechanical properties of polymer nanocomposites. Polymers 13, 2017 (2021).
-
Shereen Farhana, P., Francis, A. P., Gayathri, R., Sankaran, K. & Veeraraghavan, V. P. Synthesis and characterization of zirconium oxide nanoparticles based on hemidesmus indicus extract: evaluation of biocompatibility and bioactivity for prosthetic implant coatings. J. Adv. Oral. Res. 15, 100–108 (2024).
-
Kim, I. llY. ong, Sugino, A., Kikuta, K., Ohtsuki, C. & Cho, S. ungB. aek Bioactive composites consisting of PEEK and calcium silicate powders. J. Biomater. Appl 24, 105–118 (2009).
-
Deng, F., Wu, Liu, X., Guo, & Wei. Nano-TiO2/PEEK bioactive composite as a bone substitute material: in vitro and in vivo studies. IJN 1215 https://doi.org/10.2147/IJN.S28101 (2012).
-
Kong, F., Nie, Z., Liu, Z., Hou, S. & Ji, J. Developments of nano-TiO2 incorporated hydroxyapatite/PEEK composite strut for cervical reconstruction and interbody fusion after corpectomy with anterior plate fixation. J. Photochem. Photobiol. B: Biol. 187, 120–125 (2018).
-
Chmielewska, A. & Dean, D. The role of stiffness-matching in avoiding stress shielding-induced bone loss and stress concentration-induced skeletal reconstruction device failure. Acta Biomaterialia 173, 51–65 (2024).
-
Lin, C.-L., Wang, Y.-T., Chang, C.-M., Wu, C.-H. & Tsai, W.-H. Design criteria for patient-specific mandibular continuity defect reconstructed implant with lightweight structure using weighted topology optimization and validated with biomechanical fatigue testing. IJB 8, 437 (2021).
-
Steinbacher, D. M. Three-dimensional analysis and surgical planning in craniomaxillofacial surgery. J. Oral. Maxillofac. Surg. 73, S40–S56 (2015).
-
Dérand, P., Rännar, L.-E., Hirsch, J.-M. & Imaging Virtual planning, design, and production of patient-specific implants and clinical validation in craniomaxillofacial surgery. Craniomaxillofacial Trauma Reconstr. 5, 137–143 (2012).
-
Du, R. et al. A systematic approach for making 3D-printed patient-specific implants for craniomaxillofacial reconstruction. Engineering 6, 1291–1301 (2020).
-
Qadir, M., Li, Y., Biesiekierski, A. & Wen, C. Surface characterization and biocompatibility of hydroxyapatite coating on anodized TiO2 nanotubes via PVD magnetron sputtering. Langmuir 37, 4984–4996 (2021).
-
Van Bael, S. et al. The effect of pore geometry on the in vitro biological behavior of human periosteum-derived cells seeded on selective laser-melted Ti6Al4V bone scaffolds. Acta Biomater. 8, 2824–2834 (2012).
-
Laubach, M. et al. The concept of scaffold-guided bone regeneration for the treatment of long bone defects: Current clinical application and future perspective. JFB 14, 341 (2023).
-
Kapfer, S. C., Hyde, S. T., Mecke, K., Arns, C. H. & Schröder-Turk, G. E. Minimal surface scaffold designs for tissue engineering. Biomaterials 32, 6875–6882 (2011).
-
Verma, R. et al. Design and analysis of biomedical scaffolds using TPMS-based porous structures inspired from additive manufacturing. Coatings 12, 839 (2022).
-
Li, L. et al. The triply periodic minimal surface-based 3D printed engineering scaffold for meniscus function reconstruction. Biomater. Res 26, 45 (2022).
-
Shi, J. et al. A TPMS-based method for modeling porous scaffolds for bionic bone tissue engineering. Sci. Rep. 8, 7395 (2018).
-
Gabrieli, Wenger, R., Mazza, R., Verné, M., Baino, E. & Design, F. Stereolithographic 3D printing, and characterization of TPMS scaffolds. Materials 17, 654 (2024).
-
Karageorgiou, V. & Kaplan, D. Porosity of 3D biomaterial scaffolds and osteogenesis. Biomaterials 26, 5474–5491 (2005).
-
Hollister, S. J. Porous scaffold design for tissue engineering. Nat. Mater. 4, 518–524 (2005).
-
Turco, G. et al. Alginate/hydroxyapatite biocomposite for bone ingrowth: A trabecular structure with high and isotropic connectivity. Biomacromolecules 10, 1575–1583 (2009).
-
Huang, X. et al. Biomaterial scaffolds in maxillofacial bone tissue engineering: A review of recent advances. Bioact. Mater. 33, 129–156 (2024).
-
Song, K., Wang, Z., Lan, J. & Ma, S. Porous structure design and mechanical behavior analysis based on TPMS for customized root analogue implant. J. Mech. Behav. Biomed. Mater. 115, 104222 (2021).
-
Araya-Calvo, M., Järvenpää, A., Rautio, T., Morales-Sanchez, J. E. & Guillen-Girón, T. Comparative fatigue performance of as-built vs etched Ti64 in TPMS-gyroid and stochastic structures fabricated via PBF-LB for biomedical applications. RPJ 30, 217–230 (2024).
-
Ran, Q. et al. Osteogenesis of 3D printed porous Ti6Al4V implants with different pore sizes. J. Mech. Behav. Biomed. Mater. 84, 1–11 (2018).
-
Foroughi, A. H. & Razavi, M. J. Multi-objective shape optimization of bone scaffolds: Enhancement of mechanical properties and permeability. Acta Biomaterialia 146, 317–340 (2022).
-
Peng, W. et al. Biomechanical and Mechanostat analysis of a titanium layered porous implant for mandibular reconstruction: The effect of the topology optimization design. Mater. Sci. Eng.: C. 124, 112056 (2021).
-
Hu, B. et al. Multi-objective Bayesian optimization accelerated design of TPMS structures. Int. J. Mech. Sci. 244, 108085 (2023).
-
Gu, J. et al. Stress-driven design method for porous maxillofacial prosthesis based on triply periodic minimal surface. Composite Struct. 355, 118863 (2025).
-
Shahid, M. N., Shahid, M. U., Rasheed, S., Irfan, M. & Obeidi, M. A. Computational investigation of the fluidic properties of triply periodic minimal surface (TPMS) structures in tissue engineering. Designs 8, 69 (2024).
-
Zhang, J. et al. Machine learning guided prediction of mechanical properties of TPMS structures based on finite element simulation for biomedical titanium. Materials Technology 1–8 https://doi.org/10.1080/10667857.2021.1999558 (2021).
-
Peel, S., Bhatia, S., Eggbeer, D., Morris, D. S. & Hayhurst, C. Evolution of design considerations in complex craniofacial reconstruction using patient-specific implants. Proc. Inst. Mech. Eng. H. 231, 509–524 (2017).
-
Zhang, L., Song, B., Choi, S.-K. & Shi, Y. A topology strategy to reduce stress shielding of additively manufactured porous metallic biomaterials. Int. J. Mech. Sci. 197, 106331 (2021).
-
Moiduddin, K. et al. Structural and mechanical characterization of custom design cranial implant created using additive manufacturing. Electron. J. Biotechnol. 29, 22–31 (2017).
-
Wang, Y., Lian, Y., Wang, Z., Wang, C. & Fang, D. A novel triple periodic minimal surface-like plate lattice and its data-driven optimization method for superior mechanical properties. Appl. Math. Mech. -Engl. Ed. 45, 217–238 (2024).
-
Ji, Z., Li, D., Xie, Y. M., Zhao, Y. & Liao, W. Design and optimization of TPMS-based heterogeneous metastructure for controllable displacement field. Thin-Walled Struct. 208, 112784 (2025).
-
Kök, H. I. et al. Reduction of stress-shielding and fatigue-resistant dental implant design through topology optimization and TPMS lattices. J. Mech. Behav. Biomed. Mater. 165, 106923 (2025).
-
Zheng, N., Zhai, X. & Chen, F. Topology optimization of self-supporting porous structures based on triply periodic minimal surfaces. Comput.-Aided Des. 161, 103542 (2023).
-
Ziaie, B., Velay, X. & Saleem, W. Developing porous hip implants implementing topology optimization based on the bone remodelling model and fatigue failure. J. Mech. Behav. Biomed. Mater. 163, 106864 (2025).
-
Jitkla, N., Pinyonitikasem, A., Wiwatsuwan, P., Pairojboriboon, S. & Promoppatum, P. 3d-printed sacral reconstruction prosthesis from multiscale topology optimization: A comprehensive numerical assessment of mechanical stability. Comput. Biol. Med. 185, 109562 (2025).
-
Zhao, M., Li, X., Zhang, D. Z. & Zhai, W. TPMS-based interpenetrating lattice structures: Design, mechanical properties and multiscale optimization. Int. J. Mech. Sci. 244, 108092 (2023).
-
Luo, B., Miu, L. & Luo, Y. Titanium alloys for biomedical applications: a review on additive manufacturing process and surface modification technology. Int J. Adv. Manuf. Technol. 137, 3215–3227 (2025).
-
Alwala, A. M. et al. Analysis of the effectiveness of 3D printed patient-specific implants for reconstruction of maxillary defect secondary to mucormycosis. J. Maxillofac. Oral. Surg. 22, 728–733 (2023).
-
Rana, M. et al. Primary orbital reconstruction with selective laser melting (SLM) of patient-specific implants (PSIs): An overview of 96 surgically treated patients. JCM 11, 3361 (2022).
-
Qin, Y. et al. Additive manufacturing of Zn-Mg alloy porous scaffolds with enhanced osseointegration: In vitro and in vivo studies. Acta Biomater. 145, 403–415 (2022).
-
Salehi, M. et al. Achieving biomimetic porosity and strength of bone in magnesium scaffolds through binder jet additive manufacturing. Biomater. Adv. 166, 214059 (2025).
-
Kuah, K. X. et al. Surface modification with phosphate and hydroxyapatite of porous magnesium scaffolds fabricated by binder jet additive manufacturing. Crystals 12, 1850 (2022).
-
Singh, S., Prakash, C. & Ramakrishna, S. 3D printing of polyether-ether-ketone for biomedical applications. Eur. Polym. J. 114, 234–248 (2019).
-
Kaur, J. N., Padhi, P. & Pal, S. Biocompatible PVAc- g -PLLA acrylate polymers for DLP 3D printing with tunable mechanical properties. ACS Appl. Mater. Interfaces 16, 62594–62605 (2024).
-
Zocca, A., Colombo, P., Gomes, C. M. & Günster, J. Additive manufacturing of ceramics: Issues, potentialities, and opportunities. J. Am. Ceram. Soc. 98, 1983–2001 (2015).
-
Nayak, V. V. et al. Three-dimensional printing bioceramic scaffolds using direct-ink-writing for craniomaxillofacial bone regeneration. Tissue Eng. Part C: Methods 29, 332–345 (2023).
-
Manzoor, F. et al. 3D printed strontium and zinc doped hydroxyapatite loaded PEEK for craniomaxillofacial implants. Polymers 14, 1376 (2022).
-
Zhao, G. et al. Ti/β-TCP composite porous scaffolds fabricated by direct ink writing. Virtual Phys. Prototyp. 18, e2192703 (2023).
-
Jindal, S., Manzoor, F., Haslam, N. & Mancuso, E. 3D printed composite materials for craniofacial implants: current concepts, challenges and future directions. Int J. Adv. Manuf. Technol. 112, 635–653 (2021).
-
Moura De Souza Soares, F., Barbosa, D. M., Reis Corado, H. P., De Carvalho Santana, A. I. & Elias, C. N. Surface morphology, roughness, and corrosion resistance of dental implants produced by additive manufacturing. J. Mater. Res. Technol. 21, 3844–3855 (2022).
-
Liu, K. et al. Morphologies, mechanical and in vitro behaviors of DLP-based 3D printed HA scaffolds with different structural configurations. RSC Adv. 13, 20830–20838 (2023).
-
Wu, Y.-C., Kuo, C.-N., Chung, Y.-C., Ng, C.-H. & Huang, J. C. Effects of electropolishing on mechanical properties and bio-corrosion of Ti6Al4V fabricated by electron beam melting additive manufacturing. Materials 12, 1466 (2019).
-
Virinthorn, R. N. V. C., Chandrasekaran, M., Wang, K. & Goh, K. L. Post-process optimization of 3D printed poly(lactic-co-glycolic acid) dental implant scaffold for enhanced structure and mechanical properties: effects of sonication duration and power. J. Mater. Sci. Mater. Med. 32, 91 (2021).
-
Shaikh, S., Kedia, S., Singh, D., Subramanian, M. & Sinha, S. Surface texturing of Ti6Al4V alloy using femtosecond laser for superior antibacterial performance. J. Laser Appl. 31, 022011 (2019).
-
Han, X. et al. An in vitro study of osteoblast response on fused-filament fabrication 3D printed PEEK for dental and cranio-maxillofacial implants. JCM 8, 771 (2019).
-
Syrlybayev, D., Seisekulova, A., Talamona, D. & Perveen, A. The Post-processing of additive manufactured polymeric and metallic parts. JMMP 6, 116 (2022).
-
Pourrahimi, S. & Hof, L. A. On the post-processing of complex additive manufactured metallic parts: A review. Adv. Eng. Mater. 26, 2301511 (2024).
-
Diniță, A. et al. Additive manufacturing post-processing treatments, a review with emphasis on mechanical characteristics. Materials 16, 4610 (2023).
-
Martinez, J. S. et al. High resolution DLP stereolithography to fabricate biocompatible hydroxyapatite structures that support osteogenesis. PLoS ONE 17, e0272283 (2022).
-
Li, L. et al. Research on the dimensional accuracy of customized bone augmentation combined with 3D -printing individualized titanium mesh: A retrospective case series study. Clin. Implant Dent. Rel Res. 23, 5–18 (2021).
-
Presotto, A. G. C., Barão, V. A. R., Bhering, C. L. B. & Mesquita, M. F. Dimensional precision of implant-supported frameworks fabricated by 3D printing. J. Prosthet. Dent. 122, 38–45 (2019).
-
Tseng, P.-C. et al. Direct ink writing with dental composites: A paradigm shift toward sustainable chair-side production. Dent. Mater. 40, 1753–1761 (2024).
-
Sherman, S. L., Kadioglu, O., Currier, G. F., Kierl, J. P. & Li, J. Accuracy of digital light processing printing of 3-dimensional dental models. Am. J. Orthod. Dentofac. Orthopedics 157, 422–428 (2020).
-
Chen, S. et al. Review on residual stresses in metal additive manufacturing: formation mechanisms, parameter dependencies, prediction and control approaches. J. Mater. Res. Technol. 17, 2950–2974 (2022).
-
Zohdi, N. & Yang, R. (Chunhui). Material anisotropy in additively manufactured polymers and polymer composites: A review. Polymers 13, 3368 (2021).
-
Dadkhah, M., Tulliani, J.-M., Saboori, A. & Iuliano, L. Additive manufacturing of ceramics: Advances, challenges, and outlook. J. Eur. Ceram. Soc. 43, 6635–6664 (2023).
-
Al-Maharma, A. Y., Patil, S. P. & Markert, B. Effects of porosity on the mechanical properties of additively manufactured components: A critical review. Mater. Res. Express 7, 122001 (2020).
-
Evans, S. L. Fatigue crack propagation under variable amplitude loading in PMMA and bone cement. J. Mater. Sci Mater. Med. 18, 1711–1717 (2007).
-
Prasadh, S. et al. Biomechanics of alloplastic mandible reconstruction using biomaterials: The effect of implant design on stress concentration influences choice of material. J. Mech. Behav. Biomed. Mater. 103, 103548 (2020).
-
Qiao, Y. & Salviato, M. Micro-computed tomography analysis of damage in notched composite laminates under multi-axial fatigue. Compos. Part B: Eng. 187, 107789 (2020).
-
Lisiak-Myszke, M. et al. Application of finite element analysis in oral and maxillofacial surgery—a literature review. Materials 13, 3063 (2020).
-
Didziokas, M. et al. Multiscale mechanical characterisation of the craniofacial system under external forces. Biomech. Model Mechanobiol. 23, 675–685 (2024).
-
Guo, J. et al. Multibody dynamics modeling of human mandibular musculoskeletal system and its applications in surgical planning. Multibody Syst. Dyn. 57, 299–325 (2023).
-
Yin, M., Zhang, E., Yu, Y. & Karniadakis, G. E. Interfacing finite elements with deep neural operators for fast multiscale modeling of mechanics problems. Comput. Methods Appl. Mech. Eng. 402, 115027 (2022).
-
Garcia, S. N., Gutierrez, L. & McNulty, A. Real-time cellular analysis as a novel approach for in vitro cytotoxicity testing of medical device extracts. J. Biomed. Mater. Res 101A, 2097–2106 (2013).
-
Kheder, W. et al. Titanium Particles Modulate Lymphocyte and Macrophage Polarization in Peri-Implant Gingival Tissues. IJMS 24, 11644 (2023).
-
Gai, X. et al. A novel method for evaluating the dynamic biocompatibility of degradable biomaterials based on real-time cell analysis. Regener. Biomater. 7, 321–329 (2020).
-
Wancket, L. M. Animal models for evaluation of bone implants and devices: Comparative bone structure and common model uses. Vet. Pathol. 52, 842–850 (2015).
-
Li, Y. et al. Bone defect animal models for testing efficacy of bone substitute biomaterials. J. Orthop. Transl. 3, 95–104 (2015).
-
Wang, S. et al. Single-cell RNA sequencing reveals in vivo osteoimmunology interactions between the immune and skeletal systems. Front. Endocrinol. 14, 1107511 (2023).
-
Hatt, L. P. et al. Standard in vitro evaluations of engineered bone substitutes are not sufficient to predict in vivo preclinical model outcomes. Acta Biomater. 156, 177–189 (2023).
-
Mansoorifar, A., Gordon, R., Bergan, R. C. & Bertassoni, L. E. Bone-on-a-chip: Microfluidic technologies and microphysiologic models of bone tissue. Adv. Funct. Mater. 31, 2006796 (2021).
-
Chen, Y.-C. et al. Long-term in vitro degradation and in vivo evaluation of resorbable bioceramics. J. Mater. Sci: Mater. Med 32, 13 (2021).
-
Zeiter, S. et al. Evaluation of preclinical models for the testing of bone tissue-engineered constructs. Tissue Eng. Part C: Methods 26, 107–117 (2020).
-
Wang, J. et al. Nanostructured titanium regulates osseointegration via influencing macrophage polarization in the osteogenic environment. IJN ume 13, 4029–4043 (2018).
-
Kyllönen, L. et al. Effects of different serum conditions on osteogenic differentiation of human adipose stem cells in vitro. Stem Cell Res. Ther. 4, 17 (2013).
-
Lee, H. & Kang, K.-T. Advanced tube formation assay using human endothelial colony forming cells for in vitro evaluation of angiogenesis. Korean J. Physiol. Pharm. 22, 705 (2018).
-
Inomata, K. & Honda, M. Co-culture of osteoblasts and endothelial cells on a microfiber scaffold to construct bone-like tissue with vascular networks. Materials 12, 2869 (2019).
-
Jusoh, N., Oh, S., Kim, S., Kim, J. & Jeon, N. L. Microfluidic vascularized bone tissue model with hydroxyapatite-incorporated extracellular matrix. Lab Chip 15, 3984–3988 (2015).
-
Verbicaro, T. et al. Osteocalcin immunohistochemical expression during repair of critical-sized bone defects treated with subcutaneous adipose tissue in rat and rabbit animal model. Braz. Dent. J. 24, 559–564 (2013).
-
Tsiklin, I. L., Shabunin, A. V., Kolsanov, A. V. & Volova, L. T. In vivo bone tissue engineering strategies: Advances and prospects. Polymers 14, 3222 (2022).
-
Udagawa, A. et al. Micro- CT observation of angiogenesis in bone regeneration. Clin. Oral. Implants Res 24, 787–792 (2013).
-
Dalfino, S. et al. Regeneration of critical-sized mandibular defects using 3D-printed composite scaffolds: A quantitative evaluation of new bone formation in in vivo studies. Adv. Healthc. Mater. 12, 2300128 (2023).
-
Riehakainen, L. et al. Assessment of tissue response in vivo: PET-CT imaging of titanium and biodegradable magnesium implants. Acta Biomater. 184, 461–472 (2024).
-
Ehnert, S., Rinderknecht, H., Aspera-Werz, R. H., Häussling, V. & Nussler, A. K. Use of in vitro bone models to screen for altered bone metabolism, osteopathies, and fracture healing: challenges of complex models. Arch. Toxicol. 94, 3937–3958 (2020).
-
Negrescu, A.-M. & Cimpean, A. The state of the art and prospects for osteoimmunomodulatory biomaterials. Materials 14, 1357 (2021).
-
Taguchi, T. & Lopez, M. J. An overview of de novo bone generation in animal models. J. Orthop. Res. 39, 7–21 (2021).
-
Hatt, L. P., Thompson, K., Helms, J. A., Stoddart, M. J. & Armiento, A. R. Clinically relevant preclinical animal models for testing novel cranio-maxillofacial bone 3D-printed biomaterials. Clin. Transl. Med. 12, e690 (2022).
-
Gao, H., Huang, J., Wei, Q. & He, C. Advances in animal models for studying bone fracture healing. Bioengineering 10, 201 (2023).
-
Gulati, K. et al. Craniofacial therapy: Advanced local therapies from nano-engineered titanium implants to treat craniofacial conditions. Int J. Oral. Sci. 15, 15 (2023).
-
Wu, Y. et al. An overview of 3D printed metal implants in orthopedic applications: Present and future perspectives. Heliyon 9, e17718 (2023).
-
Gharehdaghi, N., Nokhbatolfoghahaei, H. & Khojasteh, A. 4D printing of smart scaffolds for bone regeneration: A systematic review. Biomed. Mater. 20, 012003 (2025).
-
Grunert, R. et al. Concept of patient-specific shape memory implants for the treatment of orbital floor fractures. Oral. Maxillofac. Surg. 21, 179–185 (2017).
-
Baker, R. M., Tseng, L.-F., Iannolo, M. T., Oest, M. E. & Henderson, J. H. Self-deploying shape memory polymer scaffolds for grafting and stabilizing complex bone defects: A mouse femoral segmental defect study. Biomaterials 76, 388–398 (2016).
-
Oldroyd, P., Hadwe, S. E., Barone, D. G. & Malliaras, G. G. Thin-film implants for bioelectronic medicine. MRS Bull. 49, 1045–1058 (2024).
-
Najjari, A. et al. Smart piezoelectric biomaterials for tissue engineering and regenerative medicine: a review. Biomed. Eng. / Biomedizinische Tech. 67, 71–88 (2022).
-
Memon, A. R., Li, J., Egger, J. & Chen, X. A review on patient-specific facial and cranial implant design using Artificial Intelligence (AI) techniques. Expert Rev. Med. Devices 18, 985–994 (2021).
-
Revilla-León, M. et al. Artificial intelligence applications in implant dentistry: A systematic review. J. Prosthet. Dent. 129, 293–300 (2023).
-
Drakoulas, G. et al. An explainable machine learning-based probabilistic framework for the design of scaffolds in bone tissue engineering. Biomech. Model Mechanobiol. 23, 987–1012 (2024).
-
Omigbodun, F. T. & Oladapo, B. I. AI-optimized lattice structures for biomechanics scaffold design. Biomimetics 10, 88 (2025).
-
Bose, S., Ke, D., Sahasrabudhe, H. & Bandyopadhyay, A. Additive manufacturing of biomaterials. Prog. Mater. Sci. 93, 45–111 (2018).
-
Shi, Y. et al. Influence of processing parameters on additively manufactured architected cellular metals: Emphasis on biomedical applications. JFB 16, 53 (2025).
-
Miki, T. & Yamada, T. Topology optimization considering the distortion in additive manufacturing. Finite Elem. Anal. Des. 193, 103558 (2021).
-
Yan, W. et al. An integrated process–structure–property modeling framework for additive manufacturing. Comput. Methods Appl. Mech. Eng. 339, 184–204 (2018).
-
Adak, D., Sreeramagiri, P., Roy, S. & Balasubramanian, G. Advances and challenges in predictive modeling for additive manufacturing of dissimilar metals and complex alloys. Materials 16, 5680 (2023).
-
Croom, B. P., Berkson, M., Mueller, R. K., Presley, M. & Storck, S. Deep learning prediction of stress fields in additively manufactured metals with intricate defect networks. Mech. Mater. 165, 104191 (2022).
-
Kononenko, D. Y. et al. Designing materials by laser powder bed fusion with machine learning-driven bi-objective optimization. J. Mater. Res. Technol. 30, 6802–6811 (2024).
-
Wu, C. et al. Machine learning-based design for additive manufacturing in biomedical engineering. Int. J. Mech. Sci. 266, 108828 (2024).
-
Yang, S., Wang, L., Chen, Q. & Xu, M. In situ process monitoring and automated multi-parameter evaluation using optical coherence tomography during extrusion-based bioprinting. Addit. Manuf. 47, 102251 (2021).
-
De Stefano, M. & Ruggiero, A. A critical review of human jaw biomechanical modeling. Appl. Sci. 14, 3813 (2024).
-
Seth, I. et al. Digital twins use in plastic surgery: A systematic review. JCM 13, 7861 (2024).
-
Ahn, S. et al. Toward digital twin development for implant placement planning using a parametric reduced-order model. Bioengineering 11, 84 (2024).
-
Dua, R., Jones, H. & Noble, P. C. Evaluation of bone formation on orthopedic implant surfaces using an ex-vivo bone bioreactor system. Sci. Rep. 11, 22509 (2021).
-
Khosravi, R. et al. A computational bio-chemo-mechanical model of in vivo tissue-engineered vascular graft development. Integr. Biol. 12, 47–63 (2020).
-
Ramezani, M. & Mohd Ripin, Z. 4D printing in biomedical engineering: Advancements, challenges, and future directions. JFB 14, 347 (2023).
-
Kumar, R. et al. A comprehensive review of advancements in additive manufacturing for 3D printed medical components using diverse materials. Discov. Mater. 5, 152 (2025).
-
Ritchie, R. O. The conflicts between strength and toughness. Nat. Mater. 10, 817–822 (2011).
-
International Organization for Standardization. Dentistry — Implants — Dynamic loading test for endosseous dental implants, ISO 14801:2016. (2016).
-
International Organization for Standardization. Biological evaluation of medical devices — Part 6: Tests for local effects after implantation, ISO 10993-6:2016. (2016).
-
International Organization for Standardization. Biological evaluation of medical devices — Part 5: Tests for in vitro cytotoxicity, ISO 10993-5:2017. (2017).
-
International Organization for Standardization. Biological evaluation of medical devices — Part 4: Selection of tests for interactions with blood, ISO 10993-4:2017. (2017).
-
Xu, Y. et al. Biomimetic bone-periosteum scaffold for spatiotemporal regulated innervated bone regeneration and therapy of osteosarcoma. J. Nanobiotechnol 22, 250 (2024).
-
Pujari-Palmer, M. et al. Pyrophosphate stimulates differentiation, matrix gene expression and alkaline phosphatase activity in osteoblasts. PLoS ONE 11, e0163530 (2016).
-
Dębski, T. et al. Scaffold vascularization method using an adipose-derived stem cell (ASC)-seeded scaffold prefabricated with a flow-through pedicle. Stem Cell Res Ther. 11, 34 (2020).
-
Zieliński, R. et al. Comparative evaluation of bone–implant contact in various surface-treated dental implants using high-resolution micro-CT in Rabbits’ bone. Materials 17, 5396 (2024).
-
Verbist, M. et al. Reconstruction of craniomaxillofacial bone defects with 3D-printed bioceramic implants: scoping review and clinical case series. JCM 13, 2805 (2024).
-
Selvaraj, S., Dorairaj, J. & Shivasankar, N. 3d cranial reconstruction using titanium implant – a case report. Afr. H. Sci. 22, 383–390 (2022).
-
Lee, U.-L. et al. A clinical trial to evaluate the efficacy and safety of 3D printed bioceramic implants for the reconstruction of zygomatic bone defects. Materials 13, 4515 (2020).
-
Darwich, K., Ismail, M. B., Al-Mozaiek, M. Y. A.-S. & Alhelwani, A. Reconstruction of mandible using a computer-designed 3D-printed patient-specific titanium implant: a case report. Oral. Maxillofac. Surg. 25, 103–111 (2021).
-
Li, Y. et al. Clinical application of 3D-printed PEEK implants for repairing mandibular defects. J. Cranio-Maxillofac. Surg. 50, 621–626 (2022).
-
Targońska, S. et al. Design, clinical applications and post-surgical assessment of bioresorbable 3D-printed craniofacial composite implants. Biomater. Sci. 12, 3374–3388 (2024).
Acknowledgements
Financial support from National University of Singapore (NUS) is gratefully acknowledged. (AcRF A-8000-126-00-00).
Ethics declarations
Competing interests
The authors declare no competing interests.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hou, B., Li, Y. & Wong, R.C.W. Next-generation craniomaxillofacial implants for reconstructive surgery: balancing biomechanics, biocompatibility, and bioactivity. Int J Oral Sci 18, 1 (2026). https://doi.org/10.1038/s41368-025-00410-7
-
Received:
-
Revised:
-
Accepted:
-
Published:
-
Version of record:
-
DOI: https://doi.org/10.1038/s41368-025-00410-7