Introduction
Lung infection is a relatively common clinical infectious disease, often due to lung tissue infected by pathogens (e.g., bacteria, viruses, fungi, etc.) triggered by the disease, often including bacterial pneumonia, viral pneumonia, mycoplasma pneumonia, tuberculosis, fungal infections, etc., and can be divided into two types of upper respiratory infections and lower respiratory tract infections1,2,13. In contrast, acute pulmonary infections are usually respiratory tract infections that frequently occur during emergency department visits3. As the emergency department is a gathering place for patients with various acute illnesses, there may be a variety of pathogens such as bacteria, viruses, fungi, etc., all of which can be transmitted by airborne or direct contact, which in turn can lead to pulmonary infections4. With the aging of the population and the increase in the number of patients with chronic diseases, this has led to a larger population with susceptibility, resulting in an increasing number of acute pulmonary infections5. The long-term use of antibiotics and other drugs, resulting in the gradual increase of bacterial resistance, complicates treatment efficacy, potentially leading to more severe presentations of acute pulmonary infections and underscoring the need for rapid and accurate diagnostic tools6,14. With the rapid spread of new coronaviruses and other emerging infectious diseases around the world, large-scale pulmonary infections are also caused, which also brings great pressure to the work of the emergency department. The causes of acute pulmonary infections are complex and varied, and the current situation is challenging. In order to effectively deal with acute pulmonary infections, it is necessary to strengthen infection control measures, improve the awareness and skills of medical staff on infection prevention and control, and coordinate and cooperate with other departments to deal with the challenges of acute pulmonary infections. It is also crucial to enhance the effectiveness of infection detection in the process. Current diagnostic methods include chest X-ray, computed tomography (CT), and lung ultrasound, with the latter showing promise in evaluating prognosis in settings like acute respiratory distress syndrome18.Infrared thermography, as a technology that uses infrared radiation to measure the surface temperature of an object, it can be used to display the temperature distribution of the object by converting the infrared energy radiated by an object into an image7. This technology has been widely used in many fields such as medicine, industry, and military. In industry infrared thermography can be used to detect the working condition of equipment and problems such as thermal distribution of circuit boards, overheating of electrical components etc8. Infrared thermography can also be used to observe and analyse the thermal condition of the equipment in real time, so that possible malfunctions and safety hazards can be detected in time9. Infrared thermography can also be used to detect diseases and injuries in the human body, such as breast cancer and lymphadenitis10. And in the diagnosis of lung-related diseases can also play a certain role in assisting, because different tissues and organs have different thermal properties, through the observation of thermograms can be found in abnormal areas or heat sources to analyse the results of the test, so as to provide a certain basis for the diagnosis and treatment of clinical diseases11. Therefore, this study aimed to evaluate the diagnostic efficacy of infrared thermography for emergency pulmonary infections compared to chest X-ray as the reference standard.
Materials and methods
Materials
Two hundred patients who were seen in the emergency department of our hospital from October 2020 to December 2021 were selected for this study, of which 108 patients were accompanied by pulmonary infections and 92 patients were not accompanied by pulmonary infections. Both groups of patients were tested by infrared thermography. The study complied with medical ethics standards and was approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangzhou Medical University, and informed consent was obtained and signed by the patients and their families.
Inclusion and exclusion criteria
Inclusion criteria: Patients in the infection group: Met clinical diagnostic criteria for lung infection12 AND had confirmatory findings on chest X-ray (reference standard). Clinical manifestations included chest pain, cough, sputum production, etc. Routine blood examination showed elevated leukocyte count. Auscultation revealed obvious rales in the lungs; patients’ compliance was good and they could cooperate with the study throughout the whole process; all the patients were aware of the contents of the study and signed an informed consent form.
Exclusion criteria: Patients with incomplete clinical data; patients with lung inflammation and infection caused by malignant tumours and other diseases; patients with cardio-cerebral-cerebrovascular diseases; patients with vital organ disorders and serious immune system diseases; patients with other mental disorders and communication difficulties.
Detection methods
Using X-ray examination as the gold standard, an X-ray film camera (Siemens, BLX-5) was used to conduct chest X-ray scanning for all patients. Before the test, patients were required to maintain a standing position, and line films were taken in lateral and orthogonal positions, with the voltage parameter set at 120 kV and the current parameter set at 200 mA, and the collected data were recorded in detail, and the relevant data such as the scope and degree of lung infection, as well as the impact on the surrounding tissues, etc., were collated and analysed by a professional imaging physician.
Close the doors and windows, in the room temperature of 22 ~ 25 ℃, humidity 50% ~ 65% of the closed environment without bright light using infrared thermography detection, while there is no interfering heat source, the use of non-refrigerated focal plane HYIRI-1206 non-refrigerated medical IRTI, infrared thermography can be implemented in all patients with temperature and other tests, the acquisition of the standard based on the national standard GB / T 19,665 − 2005 electronic Infrared imaging body surface thermometer general specification requirements for testing. Uncooled focal plane infrared acquisition lens 320 × 240, spectral response 8 ~ 14 μm, spatial resolution of 1.3mrad, temperature resolution of 0.05 ℃, acquisition speed of 30 frames / s, before the test, all the patients need to remove the surface clothing, the need to check the parts of the chest skin exposed, while the resting state needs to be away from the infrared lens 2 m at the same time to maintain a stable sitting position for 15 min. in standing position When taking pictures in the trunk position, the main orientation is the chest and bilateral lungs, and the operation process includes focusing, temperature calibration, image acquisition, image storage and image processing., which shows the thermal structure of the human body in the form of pseudo-colour thermograms.
Judging criteria
The distribution of infrared thermal images is usually based on the manifestation and characteristics of infrared thermal images from low to high temperatures, corresponding to the scale pseudocodes represented by different color levels, in which white is the ultra-high temperature region; red is the high temperature region; pink is the hot region; yellow is the temperature-sensitive region; green is the cool region; blue is the cold region; and black is the ultra-cold region. The sagittal line in the middle of the human body is the central axis, and the corresponding body surface part is divided according to the different levels of infrared thermal image, and the temperature value of the corresponding infrared thermal image is depicted with different temperature values from low to high temperature infrared thermal image according to the scale pseudo-code bars indicated by different colour grades, and at the same time, the temperature value of the mean temperature of the infrared thermal image of the various directions is recorded, and then the distribution of the thermal image, the change of the situation and its corresponding temperature value are qualitatively and qualitatively measured. corresponding temperature values were compared and analysed qualitatively and quantitatively. A positive IRTI finding for lung infection was defined as the presence of distinct, localized hyperthermic areas (typically appearing as red, pink, or white hotspots) over the chest/bilateral lung fields, corresponding to the regions identified on X-ray, with a measured temperature significantly higher than surrounding tissues and the corresponding area in the contralateral lung.
Statistical methods
GraphPad Prism 8.0 software was used for statistical analysis, and the measurement data conforming to normal distribution were expressed as mean ± standard deviation (x ± s), the count data were expressed by χ2 test (%), and comparisons between groups were made using independent t-tests. and the ROC curves were plotted to calculate the area under the curve (AUC), the sensitivity, the specificity and the Jordon’s index. index, and P < 0.05 indicates a statistically significant difference.
Results
General information
Upon comparison, in the comparison of basic clinical data, there were no statistically significant differences between the two groups such as gender, age, hypertension, history of alcohol consumption and smoking history (P > 0.05); however, in the combination of underlying diseases, the patients in the infected group were higher than those in the uninfected group, and the difference was statistically significant (P < 0.05), as shown in Table 1.
Comparison of infrared radiation temperature in different parts of patients in two groups
The uninfected group exhibited consistently lower temperatures across all measured regions (Table 2). Critically, infrared radiation temperatures in the infected group were significantly elevated compared to non-infected controls in the body surface (37.98 ± 1.45 °C vs. 35.87 ± 1.32 °C; t = 5.923, P = 0.001), chest (33.45 ± 1.23 °C vs. 27.15 ± 1.06 °C; t = 38.450, P < 0.001), abdomen (32.34 ± 1.36 °C vs. 28.65 ± 1.20 °C; t = 20.180, P < 0.001), bilateral lungs (36.12 ± 1.38 °C vs. 27.56 ± 1.23 °C; t = 45.940, P < 0.001), and midpoint of breasts (39.24 ± 1.83 °C vs. 30.56 ± 1.25 °C; t = 38.480, P < 0.001).
A strong positive correlation was observed between IRTI temperature differentials (ΔT) and X-ray infiltration scores (Pearson’s r = 0.89, 95% CI [0.83–0.93], P < 0.001), where infiltration scores were graded as: 0 = no opacity, 1 = < 25% lobe involvement, 2 = 25–50%, 3 = > 50%. This suggests IRTI measurements reflect radiographic disease severity.
Infrared thermography detection rate of patients in the infection group
The positive rate of infrared thermography detection in patients in the lung infection group was 93 cases (86.11%), and the positive rate of gold standard X-ray detection was 102 cases (94.44%), as shown in Table 3.
Analysis of the efficacy of infrared thermography in the detection of acute pulmonary infections
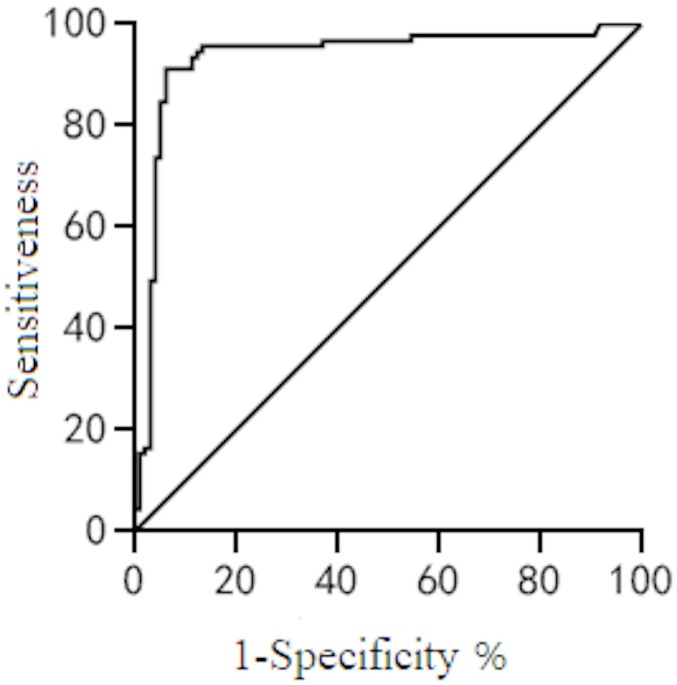
The AUC value of infrared thermography in detecting patients with acute pulmonary infections was 0.933, the sensitivity was 90.36%, the specificity was 92.28%, and the Yoden index was 0.92, suggesting that infrared thermography has good diagnostic value in acute pulmonary infections, as shown in Fig. 1.

ROC curve.
Case analysis
Case, male, 62 years old, emergency lung infection, the body surface (A: front; B: back) are seen infrared high temperature anomalous changes in phenomena, and the local performance, and showed irregular pieces and bands, and the colour shows abnormal, and has the distribution of the pattern of the meridian, as shown in Fig. 2.
Non-infected patients consistently showed homogeneous temperature distribution over the thorax (mean 33.5 °C ± 1.2 °C, range 32.1–35.0 °C), with < 0.5 °C variation between bilateral lung fields. This contrasts sharply with infected cases exhibiting localized hyperthermia (> 37 °C) and > 2 °C asymmetry (Fig. 2; Table 2). Representative normal thermal ranges are further documented in public repositories.

Case Analysis.
Discussion
Our study demonstrates that infrared thermography (IRTI) effectively identifies significant surface temperature elevations in key anatomical regions (body surface, chest, abdomen, bilateral lungs, midpoint of breasts) among emergency patients with pulmonary infections compared to non-infected controls. These findings align with the known pathophysiology, where inflammation caused by infection increases local metabolic activity and blood flow, generating detectable heat signatures16. The observed temperature differences were substantial and statistically significant (P < 0.05, Table 2), reinforcing IRTI’s potential as a physiological indicator of infection. IRTI’s rapid turnaround and safety profile make it suitable for initial screening during outbreaks or in resource-limited settings where CT is unavailable.
The diagnostic performance metrics of IRTI were robust. An AUC of 0.933 indicates excellent discriminatory ability19. The sensitivity (90.36%) and specificity (92.28%) suggest IRTI is effective in both correctly identifying infected patients and ruling out infection in non-infected individuals. The high Youden’s index (0.92) further supports its overall diagnostic utility. While the IRTI positive rate (86.11%) was slightly lower than the X-ray gold standard rate (94.44%), the difference was statistically significant (P = 0.039, Table 3). This discrepancy warrants consideration. Potential explanations include:
Technical/Interpretation factors
Deep-seated infections or those with minimal surface temperature change might be less detectable by IRTI. Operator experience and precise interpretation criteria are crucial11,15.
X-ray sensitivity
Chest X-ray, while our reference standard, has known limitations in sensitivity, particularly for early or subtle infiltrates18. Some X-ray positive cases might represent pathologies with minimal associated inflammation detectable by IRTI.
Timing
The stage of infection and prior treatment could influence the inflammatory response and thus the thermal signature.
While this study demonstrates IRTI’s diagnostic value through quantitative temperature analysis (Table 2), representative thermal images of non-infected patients were not included due to institutional ethical restrictions protecting control-group confidentiality. However, the homogeneous temperature distribution in non-infected individuals (< 1.5 °C variation across lung fields, Table 2) provides objective evidence of the absence of inflammatory hyperthermia, serving as a functional biomarker. Future studies with explicit consent for image sharing may further visualize this contrast.
Our findings corroborate previous research exploring IRTI in respiratory conditions. Studies have shown its ability to detect temperature changes associated with acute upper respiratory tract infections19 and its potential in monitoring inflammatory responses. The significant temperature elevations we observed over bilateral lungs and the chest midline specifically validate its relevance for pulmonary pathology detection11,16. The case example (Fig. 2) visually demonstrates the characteristic irregular, hyperthermic patterns associated with infection, contrasting with the uniform pattern seen in a non-infected patient.
The advantages of IRTI in the emergency setting are notable: it is rapid, non-invasive, non-contact (reducing cross-infection risk)15, radiation-free, and provides a physiological correlate of inflammation. These features make it particularly suitable for initial screening, triage, monitoring treatment response, and potentially for patients where repeated radiation exposure is a concern17. However, its role is likely complementary rather than substitutive. It cannot provide the anatomical detail of X-ray or CT, nor the functional and bedside utility of lung ultrasound18.
Conclusion
Infrared thermography demonstrates significant value as a diagnostic tool for emergency pulmonary infections. It reliably detects localized hyperthermia associated with lung infection, showing excellent discriminatory power (AUC 0.933), high sensitivity (90.36%), and specificity (92.28%). Its non-invasive, rapid, and radiation-free nature makes it particularly suitable for the emergency department environment, offering potential for use in initial screening, triage, and monitoring therapeutic response. While not replacing anatomical imaging like X-ray or CT, IRTI provides valuable physiological information reflecting inflammatory activity. Future studies should explore its integration with other modalities like lung ultrasound and its application in specific patient subgroups or emerging pathogens.
Limitations
The reliance on X-ray as the sole gold standard is a limitation, as chest CT is more sensitive, particularly for early or subtle pneumonias. Some patients classified as non-infected based on X-ray might have had CT-detectable infections, potentially biasing the control group18.Environmental control, while standardized, can still influence surface temperatures. Strict adherence to protocol is essential.The study population was from a single center. Multi-center validation would strengthen generalizability. IRTI interpretation, while based on defined criteria, has a subjective component. While chest X-ray served as our practical reference standard, computed tomography (CT) is recognized to have higher sensitivity for detecting early or subtle pneumonias. The observed 94.44% X-ray detection rate may underrepresent true infection prevalence, potentially affecting IRTI’s apparent specificity20. Further standardization of analysis protocols is beneficial. Future multicenter studies with CT correlation are needed to validate these findings. This study did not stratify patients by pneumonia type (typical/atypical). Future studies should evaluate IRTI’s performance across different etiologies.
Data availability
This statement will replace any previous statements written within the manuscript and is the definitive one that we will publish regarding data availability.The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Please refer to our Data availability statements page for further guidance and examples. All authors confirm that they have full access to the data and take full responsibility for its integrity and accuracy.
References
-
Cheng, L. et al. Co-infection of Pneumocystis jirovecii pneumonia and pulmonary CMV in a infant with X-linked severe combined immunodeficiency. Diagn. Cytopathol. 49 (9), E340–E343 (2021).
-
Fairchild, R. M. et al. Prevalence and significance of pulmonary disease on lung ultrasonography in outpatients with SARS-CoV-2 infection.bmj. Open. Respir Res. 8 (1), e000947 (2021).
-
Wang, W. Y. et al. Pulmonary cladosporium infection coexisting with subcutaneous Corynespora Cassiicola infection in a patient:a case report. World J. Clin. Cases. 10 (11), 3490–3495 (2022).
-
Zanchi, S. et al. A reproducible sensor pattern to suspect COVID19 pulmonary infection with LATITUDE. Case report and literature review. Pacing Clin. Electrophysiol. 45 (3), 425–430 (2022).
-
Zhang, X. et al. Klebsiella pneumoniae infection associated septic pulmonary embolism in an emergency department from East China. Ann. Palliat. Med. 10 (2), 1521–1529 (2021).
-
Jeican, I. I. et al. COVID-19 and Pneumocystis jirovecii pulmonary Coinfection-The first case confirmed through autopsy. Med. (Kaunas). 57 (4), 302 (2021).
-
Vergilio, M. M. et al. Evaluation of skin using infrared thermal imaging for dermatology and aesthetic applications. J. Cosmet. Dermatol. 21 (3), 895–904 (2022).
-
Huo & Chengjun Shi Yilong,Wu Xiaolei,et al. Target detection method for electrical equipment based on thermal imaging. Laser and Infrared,2021,51(4):530–536.
-
Otsuka, M. et al. Real-time monitoring of tablet surface temperature during high-speed tableting by infrared thermal imaging. J. Drug Deliv Sci. Technol. 1 (8), 102736 (2021).
-
Mei, G. et al. The influence of high temperature weather on human body temperature measurement by infrared thermal imaging thermometer. J. Phys. Conf. Ser. 2112 (1), 012024 (2021).
-
Levman, J. E. On digital infrared thermal imaging for breast cancer detection. BMJ 5 (1), 115–116 (2021).
-
Emergency Physicians Branch of the Chinese Physicians Association Expert consensus on clinical practice of emergency severe pneumonia in China. China Emerg. Med. 36 (2), 97–107 (2016).
-
Wit, K. D. et al. Comparison of YEARS and Adjust-Unlikely D-dimer testing for pulmonary embolism in the emergency department. Ann. Emerg. Med. 81 (5), 558–565 (2023).
-
Sarah, H. et al. Potential long-term effects of SARS-CoV-2 infection on the pulmonary vasculature: a global perspective. Nat. Rev. Cardiol. 19(5):314–331(2022) .
-
Kelly-Hope, L. A. et al. Infrared thermal imaging as a novel Non-Invasive Point-of-Care tool to assess filarial lymphoedema. J. Clin. Med. 10 (11), 2301 (2021).
-
Grozdanova-Uzunova, R. Infrared thermography in the diagnostics of hidden infections -case reports[J]. J. Phys. Conf. Ser. 1859 (1), 012040 (2021).
-
Wei, X. et al. Infrared thermography-based exploration of the effects of sound-induced Qi on Qi changes of the five viscera. Chin. J. Traditional Chin. Med. 36(6):3314–3317(2021) .
-
Yang, Y., Wang, M. & Liu, B. Evaluation of the prognosis of patients with acute respiratory distress syndrome at the emergency department based on the lung ultrasound score. J. Ultrasound Med. 42 (5), 1123–1131. https://doi.org/10.1002/jum.16145 (2023).
-
Zhang, Z. et al. Precise analysis of infrared thermograms of acute upper respiratory tract infection based on infrared thermography. Lingnan J. Emerg. Med. 26 (3), 247–250 (2021).
-
Zhu, J. et al. Evaluation of the clinical efficacy of painless bee therapy based on infrared thermography in the treatment of lung and spleen Qi deficiency type allergic rhinitis. J. Extern. Treat. Traditional Chin. Med. 31 (2), 27–29 (2022).
Funding
The study was funded by the following two project: 1.Accurate localization, qualitative and quantitative study of infrared thermal imaging in patients with acute upper respiratory tract infection, Project Number: A2018305; 2. Expression analysis and clinical grading of cobra bite wound by infrared thermal imaging (National Innovation and Entrepreneurship Training Program Project for College Students), Project Number: 202010570004.
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Z., Cao, Z., Wu, Z. et al. Analysis of the value of infrared thermal imaging technology in the diagnosis of emergency pulmonary infections. Sci Rep 15, 29278 (2025). https://doi.org/10.1038/s41598-025-15123-4
-
Received:
-
Accepted:
-
Published:
-
DOI: https://doi.org/10.1038/s41598-025-15123-4