
Introduction
Air leak is a common complication of lung resection, leading to longer hospital say and increased costs1. Prolonged air leaks have been studied in terms of patient background risks2,3,4, intraoperative repairs5,6, postoperative repairs1,7, and differences among drainage systems8. The water submersion test (W-test) is widely used for detecting intraoperative air leaks but has limitations: [1] subjective judgment; [2] difficulty in detection due to small surgical space in patients with emphysema, obstructive pulmonary disease, or intrathoracic adhesions; [3] potential vagal responses from cold water; [4] poor visibility due to cloudiness when using saline; [5] tissue damage from distilled water9; [6] oversight in insufficient lung expansion10,11; and [7] administered water flowing to the unaffected side in patients with interthoracic communication12. These drawbacks are more pronounced in the video-assisted thoracoscopic surgery (VATS)10,11. However, to the best of our knowledge, no other method currently matches the W-test for detecting intraoperative air leaks. From the experience of smelling gas anaesthetics in air leak cases, we assumed that examining gas components in the thoracic cavity could allow air leak detection and reduce oversight. We investigated the relationship between intraoperative alveolar air leakage by the W-test and the measurement of intrathoracic gas concentrations (G-test). This study’s hypotheses were1: all gas concentrations increase in positive patients with a positive W-test, and2 if gas concentrations increase in patients with a negative W-test, it indicates an overlooked air leak.
Methods
Ethical statement
This single-centre prospective study was presented in accordance with the STROBE Reporting Checklist and registered in the UMIN Registry (UMIN000016006, 19/12/2014). It was conducted in accordance with principles of the Declaration of Helsinki (revised 2013), and was approved by the Ethics Committee of the Joetsu General Hospital (J-77). All patients provided written informed consent prior to study participation.
Inclusion and exclusion criteria
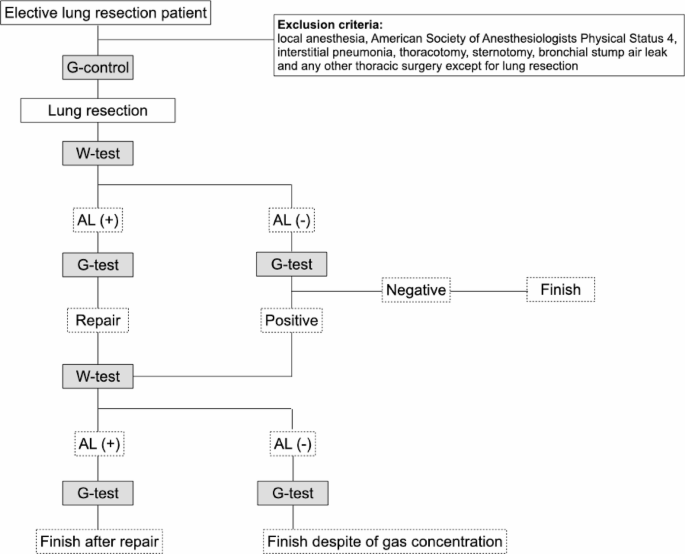
This study included all patients who underwent elective lung resections at Joetsu General Hospital (Joetsu, Niigata) between November 2013 and May 2015. The exclusion criteria were: local anaesthesia, American Society of Anaesthesiologists Physical Status 4, interstitial pneumonia, thoracotomy, sternotomy, bronchial stump air leak, any thoracic surgery except lung resection, and missing data.
Preoperative tests
All patients underwent chest X-ray, computed tomography, blood tests, urine tests, electrocardiograms, and pulmonary function tests. Cerebral magnetic resonance imaging and positron emission tomography were performed in patients with lung cancer. Patients aged 80 years or more underwent preoperative echocardiography and exercise stress testing.
Anaesthesia
Anaesthesia was managed using a combination of general anaesthesia and thoracic epidural anaesthesia. Following placement of the epidural catheter in the awake patient, general anaesthesia was initiated with a bolus administration of propofol (1.0–2.0 mg/kg) and fentanyl (50–100 µg), followed by a continuous infusion of remifentanil (0.25–0.5 µg/kg/min). After a bolus of rocuronium (0.6–1.0 mg/kg) to achieve muscle relaxation, the airway was secured using a double-lumen endotracheal tube (35–37 Fr. Blue line endobronchial tube for left lung, PORTEX, Smiths Medical, USA) for single-lung ventilation. After positioning the patient laterally, bronchoscopy confirmed the endobronchial tube position: the affected side tube was clamped, and auscultation confirmed the position. Single-lung ventilation was maintained at ETCO2 35–45 mmHg and a maximum airway pressure of 18 cmH2O using pressure control mode. Positive end-expiratory pressure was not applied. General anaesthesia was maintained with desflurane (Des), remifentanil, and rocuronium. Des was adjusted between 40 and 60 using the bispectral index (BIS Brain Monitoring System, COVIDIEN, USA).
Surgical procedure
Partial lung resection was performed using three-port VATS, with an additional 5-mm port for lobectomy and segmentectomy. The ports utilized an AESCULAP Flexibile trocar (B-Braun, Germany). A thoracoscope with a 30-degree, 5- or 10-mm camera was used. All surgeries were performed by the same surgeon.
Intraoperative air leak test
The W-test and G-test were performed according to the procedure described below (Fig. 1).

The study flowchart. AL, air leak; Des, desflurane; G-control, intrathoracic gas concentration in control; G-test, intrathoracic gas concentration in air leak test; W-test, water leak test.
1. G-control
For the measurement of intrathoracic gas concentrations, the inhaled gases were fixed (oxygen (O2) 5 L/min, Des 5.0%, FiO2 equivalent to 95%) and airway pressure maintained at 15 cmH2O for at least 5 min before measurement. Thoracoscopic ports were placed, the thoracic cavity was observed, and the affected lung was confirmed to be sufficiently collapsed and unventilated. Intrathoracic gas components were measured before lung parenchyma operation. The sampling tube of the multi-gas channel of the anaesthesia gas monitor (Lifescope, NIHON KOHDEN, Japan) was removed from the anaesthesia machine. An extension tube (50 cm, Suffed, TERUMO, Japan) of a 12 Fr. suction catheter (NIPRO, Japan) and a tracheal suction kit (MD-33050, Sumitomo Bakelite, Japan) for water trapping were connected to the sampling tube. A 12 Fr. suction catheter was inserted into the thoracic cavity from one port, and intrathoracic gases were continuously collected and measured (Fig. 2A). Baseline levels of Des. (%), O2 (%), and carbon dioxide (CO2) (mmHg) were recorded 1 min after starting intrathoracic gas sampling (Fig. 2B). During gas collection, the surgeon manually blocked other ports to prevent air inflow into the thoracic cavity.

Intrathoracic gas measurement. Display of gas concentration. A sampling tube connected to the gas analyser of the anaesthesia machine was connected to a tracheal suction kit as a water trap (yellow arrow), and a 12 Fr. suction catheter. It is inserted into the thoracic cavity through the port (red arrow). During measurement, all ports were closed with a finger (black arrow). This photograph shows a case of intrathoracic gas concentration as FiCO2 and FiO2 FiDES in the control measurements (yellow circle).
2. W-test
Warm distilled water (1 L) was administered to the thoracic cavity after specimen removal. After re-inflating the operated lung (peak pressure 15 cmH2O), the location of any fistula was identified. Bronchial stump air leaks were excluded in this study. Alveolar air leaks were rated as follows: 0, none; 1, mild, characterized by non-coalescent single bubbles; 2, moderate, characterized by intermittent coalescent single bubbles; and 3, severe air leak with coalescent bubbles or multiple air leaks. Rating was based on surgeon-anaesthesiologist agreement. After the W-test, a G-test was performed without fistula repair.
3. G-test
After aspirating distilled water, both lungs were continuously re-pressurized at 15 cmH2O. Intrathoracic gas concentrations were measured then as in the G-control after 1 min of pressurization. We assumed a G-test positive if their G-test values were higher than the G-control value at least two gases. If the initial G-test was positive but the W-test was negative, only the W-test was repeated for the second test to minimize potential lung damage from further inflation.
Air leak repair
For mild leaks, the fistula was covered with a polyglycolic acid sheet (Neoveil, Gunze, Japan) and fibrin glue6. For severe leaks, the fistula was sutured with 4 − 0 Prolene (Ethicon, USA) and covered with a polyglycolic acid sheet and fibrin glue.
Chest tube management
A 20 Fr. chest tube was used with a Thopaz (Medela, Switzerland) and controlled at − 10 cmH20. The tube was removed when drainage was < 200 mL/day, and air leak was < 10 mL/min for over 12 h.
Variables and assessments
The primary endpoint was the association between intraoperative alveolar air leakage assessed by the W-test and intrathoracic gas concentrations evaluated by the G-test.
Patient and surgical characteristics, as well as follow-up parameters, were recorded from the preoperative period to 3 months after surgery. This included age, sex, past medical history, smoking history, body mass index, estimated glomerular filtration rate, spirometry-measured respiratory function, diagnosis, diseased side, emphysema, procedure type (partial resection, segmentectomy, lobectomy), intraoperative bleeding, W-test, G-test, operative time, chest tube duration, and complications (including prolonged air leak ≥ 5 days). Complications were defined as any deviation from the expected postoperative course and graded according to the Clavien–Dindo classification13. Diagnoses of interstitial lung diseases were confirmed based on a combination of clinical and radiological findings following the 2011 guidelines of the American Thoracic Society14.
Data management and statistical analysis
This prospective study investigated data collected from the Joetsu General Hospital. Surgical procedures, anaesthesia management, and data measurements were performed by the surgeon and four anaesthesiologists.
The sample size was calculated based on previous studies and our experience with the frequency of prolonged air leak5,6,15,16. We expected to include 25% of patients with intraoperative alveolar air leaks in this study. Considering a statistical power of 80% and significance level of 5% (one-arm), the sample size was estimated to be 95. Expecting a dropout rate of 20%, we aimed to recruit 114 patients.
Continuous variables are presented as means with interquartile ranges (IQRs) for normally and non-normally distributed data, respectively. Categorical variables are presented as numbers (percentages). Air leaks that occurred after returning to the ward were not included in the analysis. The relationship between the number of bubbles in the W-test and the intrathoracic gas concentration in the G-test was evaluated using the correlation coefficient.
The prognostic value of the intraoperative air leak test was evaluated using its sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy to predict the outcome in the dataset. These analyses were performed based on the results of the first and second W-test and each intrathoracic gas measurement of the G-test. In this analysis, the G-test was considered positive only when all three gas types were elevated. Air leaks were defined as present if the W-test yielded a positive result or if air leaks were observed immediately after wound closure before the patient left the operating room. Air leaks that occurred after the patient returned to the ward were not included from this analysis. Based on these results, we calculated the sensitivity, specificity, PPV, and NPV of each test.
All statistical analyses were performed using JMP version 16.0 (SAS Institute Inc., Cary, NC, USA).
Results
Of 114 patients initially considered, 88 were enrolled due to 26 dropouts (Fig. 3; Table 1). In the G-control, no increases in Des or O2 were observed. The median CO2 concentration was 1.0 mmHg [IQR: 1–2 mmHg], which was higher than the atmospheric pressure.

The patient flowchart. Postop. AL, postoperative air leak; PPAL, postoperative prolonged air leak; Des, desflurane; G-control, intrathoracic gas concentration in control; G-test, intrathoracic gas concentration in air leak test; W-test, water leak test.
Intrathoracic O2 as a primary indicator for air leak detection
The W-test was positive in 32 of 88 cases (36.3%), with air bubbles of 1.5 degree [IQR: 1.0–3.0 degree]. Among these 32 patients, the G-test revealed elevated concentrations of all three gases in 31 cases (96.9%). After air leas site repair, all four cases that remained positive on the 2nd W-test again showed elevated levels of all gases in the 2nd G-test. Additionally, two patients with negative 2nd W-test also showed all gases elevated in the 2nd G-test, indicating immediate postoperative air leaks despite the W-test result.
Notably, the single patient with a positive W-test and intermittent, small air bubbles only showed elevated CO2 (5 mmHg). Aside from this specific patient, all other negative W-test cases exhibited either no elevated gas concentration, elevated CO2 only, or elevated CO2 and Des. No isolated Des, O2, O2/CO2, or O2/Des increases were observed, emphasizing the robust association of intrathoracic O2 with the presence of air leak (Table 2).
Correlation and test performance
Intrathoracic gas concentrations positively correlated with the degree of air bubbles on the W-test (Des r = 0.84, O2 r = 0.80, and CO2 r = 0.77) (Fig. 4).

Correlation between W-test and G-test. A positive correlation was found between the number of air bubbles in the W-test and intrathoracic gas in the G-test. The correlation coefficients for CO2 were γ = 0.77, for O2 γ = 0.80, and for Des γ = 0.84. Even if the W-test was negative, there were cases in which intrathoracic gas increased. G-test, intrathoracic gas concentration in air leak test; W-test, water leak test; Des, desflurane.
The total W-test demonstrated a sensitivity of 78.2%, a specificity of 100%, a PPV of 100%, and a NPV of 87.9%. The G-test demonstrated a sensitivity of 97.8%, a specificity of 100%, a PPV of 100%, and a NPV of 98.6% (Table 3).
Prolonged air leak cases
Two patients with air leaks ≥ 5 days required pleurodesis. In one patient (right upper lobectomy, emphysema), the W-test remained positive after initial repair, necessitating a second repair. The other patient (right upper lobectomy and middle lobe partial resection) had a negative initial W-test, but the 2nd W-test was positive due to ≥ 2 elevated gases on the G-test.
Discussion
This study demonstrated that positive W-tests correlated with higher intrathoracic gas levels (CO2, O2, Des) during air leaks. All leaks showed elevation of all three gases in the G-test. Especially, 10 patients with negative W-test but with elevated all gases, all of whom showed air leaks after skin closure. Among the gaseous components, elevated intrathoracic O2 concentration suggested air leaks. Our findings supported the experience of volatile anaesthetics odor for air leak detection. The G-test may be as effective or superior to the W-test. It would be particularly valuable in cases with W-test limitations (severe emphysema, severe intrathoracic adhesions, or interthoracic communication). In short, rising intrathoracic O2 would suggest air leaks, even with negative W-test.
The intrathoracic O2 detection could work even with total intravenous anaesthesia, avoiding volatile anaesthetics. Since propofol widely has individual variations in blood concentration, anaesthetic depth needs to be monitored; however, this is easier to control with Des. Des offers straightforward administration via general anaesthesia machines and does not require an additional machine, so we routinely use Des in our hospital. There are global calls to phase out the use of Des due to its greenhouse effect. Consequently, Des is expected to be discontinued in the future. Moreover, Des detection is not essential for G-test, as O2 concentrations alone can adequately supplement the results.
Pre-resection intrathoracic gas (G-control) was expected to match atmospheric concentrations, only increasing only during air leaks. However, median intrathoracic CO2 in the G-control showed 1.0 mmHg, exceeding atmosphere levels (below 0.5 mmHg, undetectable by the gas analyser). Additionally, 43 cases with negative W-test had elevated CO2, and 2 had elevated CO2 and Des. This suggested CO2 diffusion from the pleural tissue into the thoracic cavity. Diffusion capacity of gas through a biological membrane within a unit time is expressed by the equation: Diffusing capacity = (SA x ΔP x Sol)/{h x (MW) 1/2 }, (SA, surface area of the membrane exposed to gas; ΔP, the partial pressure gradient of the gas between tissue and chest cavity; Sol, the gas’s membrane solubility; h, the membrane thickness; MW, the gas’s molecular weight)17.
Pleural diffusion is over 10 times less efficient than gas exchange in the alveolar membrane18. G-control detected intrathoracic CO2 in most cases. However, Des and O2 absence in G-control likely related to their differing partial pressure, solubility, and molecular weight compared to CO2. Assuming similar membrane solubility to water19, the solubility of each gas in water per unit volume is 0.275 for Des, 0.024 for O2, and 0.57 for CO2 at human body temperature19,20. Therefore, the amount of diffused CO2 is approximately 20 times and 4 times higher than O2 and Des.
O2 detection was also affected by the small difference in partial pressure between tissue oxygen and atmospheric oxygen. Partial pressure of arterial oxygen (PaO2) is approximately 100–250 mmHg even with fraction of inspiratory oxygen (FiO2) 1.0, decreasing further during transport to peripheral tissues21,22,23. Therefore, the partial pressure of O2 in the peripheral lung tissue is lower than that of PaO2, with a small difference (approximately 160 mmHg in room air). This could also relate to the fact that the affected lung almost collapses and shunt formation in the G-control group. Because the O2 display of the gas analyser used in this study is rounded off to the first decimal place, detecting ≥ 22% intrathoracic O2 via diffusion is theoretically improbable24,25.
Des diffusion is one-quarter that of CO2, and Des was undetectable in G-control19,20. Increased pleural surface area likely could explain the two W-test negative cases with elevated G-test CO2 and Des. This is supported by the elevated CO2 (median 1.0 mmHg [IQR: 1–2]) in G-control, suggesting a larger inflated lung pleural surface area. Inhaled Des was reported to diffuse through the pleura, peritoneum, and skin over time; therefore, the time effect may also be relevant26,27.
G-test under 15 cmH2O pressure effectively correlated air bubbles (W-test) with intrathoracic gas, but the relationship between the degree of pressurization and air leak detection was not examined in this study. While the current G-test cannot pinpoint the leak site, its key role is not missing air leaks3,28. Addressing intraoperative air leaks significantly impacts postoperative outcomes. This research aimed to overcome the limitations of the W-test using the G-test. While the G-test currently cannot identify the exact fistula, the location can be estimated from the resected stump. Therefore, determining whether to use sealants based on the G-test could avoid unnecessary medical resources. In cases of secondary pneumothorax, not only sealants but intrathoracic pleurodesis may also be a viable option29. Postoperative persistent air leaks are influenced by risk factors such as COPD, upper lobectomy, and male sex; hence, they may still occur despite intraoperative intervention1.
The W-test classification system is subjective. There is no established method for the quantitative evaluation or a unified classification system for the W-test30, highlighting the significance of our research in providing a quantitatively assessment of air leaks using the G-test. Future intraoperative air leak management (sealants, suturing, observation) may become clearer based on G-test. Additionally, coloured and visible anaesthetic gases may be developed to identify the fistula.
Limitations
This study has several limitations. It was a single-centre study with a limited number of cases and anaesthesia management. However, the reproducibility would be high due to the standardized procedures and evaluations. Pressurization was maintained at 15 cmH2O, but results might differ with 20 cmH2O. However, the correlation between air leaks and intrathoracic gas concentrations would be unchangeable. Repeating W-test and G-test could potentially cause secondary lung damage. If the first W-test yielded a negative result and the G-test was positive, a second G-test was not conducted. Additionally, this study’s hypotheses were1: all gas concentrations increase in positive patients with a positive W-test, and2 if gas concentrations increase in patients with a negative W-test, it indicates an overlooked air leak. The methodology was based on these hypotheses.
This study did not fully examine the relationship between the G-test and postoperative prolonged air leak, and included postoperative Thopaz data. Future studies should include detailed postoperative Thopaz data to confirm the correlation with the postoperative course. This study used O2, CO2, and Des. Considering the greenhouse effect, reducing Des use is necessary, and our findings suggest that it can be replaced with O2 alone. Future studies will explore this with intravenous anaesthesia.
The W-test and G-test were performed in the lateral decubitus position. Further studies should investigate different positions as air leaks may stop spontaneously due to positional or ventilation changes. G-test’s higher sensitivity may the possibility of overestimation and unnecessary repair.
Finally, due to some dropouts, the intended sample size was not met. However, since there is no previous research in this area, this study incorporates elements of a pilot study. Therefore, prospective, multicenter clinical trials with larger cohorts would be required in the future.
Conclusions
Intrathoracic gas concentration measurements could be a useful alternative or complementary method to W-test for detecting intraoperative air leaks. Elevated intrathoracic O2 concentration was more likely to indicate air leaks. The G-test could be one method for screening air leaks, particularly in cases where the W-test is technically challenging or in patients with a negative W-test but a high clinical suspicion of air leakage.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request after approval from the Ethical Committee of the Joetsu General Hospital. The period end 3 months to 3 years after the publication.
Abbreviations
- W-test :
-
water submersion test
- VATS :
-
video-assisted thoracoscopic surgery
References
-
Sakata, K. K., Reisenauer, J. S., Kern, R. M. & Mullon, J. J. Persistent air leak – review. Respir Med. 137, 213–218 (2018).
-
Rivera, C. et al. Characterization and prediction of prolonged air leak after pulmonary resection: a nationwide study setting up the index of prolonged air leak. Ann. Thorac. Surg. 92, 1062–1068 (2011).
-
Kim, W. H., Lee, H-C., Ryu, H-G., Yoon, H-K. & Jung, C-W. Intraoperative ventilatory leak predicts prolonged air leak after lung resection: A retrospective observational study. PLoS One. 12, e0187598 (2017).
-
Homma, T. et al. Utility of the sliding lung sign for the prediction of preoperative intrathoracic adhesions. J. Thorac. Dis. 12, 4224–4232 (2020).
-
Malapert, G., Hanna, H. A., Pages, P. B. & Bernard, A. Surgical sealant for the prevention of prolonged air leak after lung resection: meta-analysis. Ann. Thorac. Surg. 90, 1779–1785 (2010).
-
Kawai, H., Harada, K., Ohta, H., Tokushima, T. & Oka, S. Prevention of alveolar air leakage after video-assisted thoracic surgery: comparison of the efficacy of methods involving the use of fibrin glue. Thorac. Cardiovasc. Surg. 60, 351–355 (2012).
-
Hugen, N., Hekma, E. J., Claessens, N. J. M., Smit, H. & Reijnen, M. Efficacy of an autologous blood patch for prolonged air leak: a systematic review. Ann. Thorac. Surg. 114, 106471 (2021). S0003-4975(21)01005-5.
-
Gilbert, S. et al. Randomized trial of digital versus analog pleural drainage in patients with or without a pulmonary air leak after lung resection. J. Thorac. Cardiovasc. Surg. 150, 1243–1249 (2015).
-
Takiyama, S., Kono, Y., Horishita, T. & Kawasaki, T. A case of transient ST elevation following intrathoracic distilled warm water irrigation after pericardiotomy during thoracic surgery. JJSCA 40, 128–134 (2020). (in Japanese).
-
Barker, A., Maratos, E. C., Edmonds, L. & Lim, E. Recurrence rates of video- assisted thoracoscopic versus open surgery in the prevention of recurrent pneumothoraces: a systematic review of randomised and non-randomised trials. Lancet 370, 329–335 (2007).
-
Scanagatta, P., Sestini, S., Duranti, L. & Piccioni, F. eComment. A bicycle inner tube in a glass of water! Video-assisted thoracoscopic surgery for spontaneous pneumothorax and the submersion test. Interact. Cardiovasc. Thorac. Surg. 20, 652–653 (2015).
-
Homma, T., Tsuji, T., Shimada, Y., Tanabe, K. & Shida, K. Bilateral pneumothorax due to the interthoracic communication with poor ventilation resulted from water submersion test. Hokuriku J. Surg. 40, 23–26 (2022). (in Japanese).
-
Dindo, D., Demartines, N. & Clavien, P. A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 240, 205–213 (2004).
-
Raghu, G. et al. An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis: evidence-based guidelines for diagnosis and management. Am. J. Respir Crit. Care Med. 183, 788–824 (2011).
-
Homma, T. et al. Risk factors of neuropathic pain after thoracic surgery. J. Thorac. Dis. 10, 2898–2907 (2018).
-
Homma, T. et al. Efficacy of 50 mg Pregabalin for prevention of postoperative neuropathic pain after video-assisted thoracoscopic surgery and thoracotomy: a 3-month prospective randomized controlled trial. J. Thorac. Dis. 11, 694–701 (2019).
-
Kavanagh, B. & Hedenstierna, G. Miller’s Anesthesia 8th edition: Chap. 19. Respiratory physiology and pathophysiology455–456 (Elsevier, 2018).
-
Berne, R. B. & Levy, M. N. Physiology 2nd edition: Chap. 39. Gas Exchange and Gas Transport. C.V. Mosby :605–623. (1988).
-
Guyton, A. C. & Hall, J. E. Textbook of Medical Physiology: Chap. 39. Physical Principles of Gas Exchange; Diffusion of Oxygen and Carbon Dioxide Through the Respiratory Membrane491–501 (Elsevier, 2006).
-
Esper, T., Wehner, M., Meinecke, C. D. & Rueffert, H. Blood/Gas partition coeffficients for isoflurane, sevoflurane, and desflurane in a clinically relevant patient population. Anesth. Analg. 120, 45–50 (2015).
-
Rees, D. I. & Wansbrough, S. R. One-lung anaesthesia: percent shunt and arterial oxygen tension during continuous insufflation of oxygen to the nonventilated lung. Anesth. Analg. 61, 507–512 (1982).
-
Rees, D. I. & Gaines, G. Y. 3rd One-lung anaesthesia–a comparison of pulmonary gas exchange during anaesthesia with ketamine or enflurane. Anesth. Analg. 63, 521–525 (1984).
-
Peel, J. K., Funk, D. J., Slinger, P., Srinathan, S. & Kidane, B. Positive end-expiratory pressure and recruitment maneuvers during one–lung ventilation: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 160, 1112–1122 (2020).
-
Ernstene, A. C. & Volk, M. C. Cutaneous respiration in man: VI. The effect of drugs on the rate of carbon dioxide elimination and oxygen absorption. J. Clin. Invest. 11, 383–386 (1932).
-
Ernstene, C. & Volk, M. C. Cutaneous respiration in man: VII. The effect of venous congestion on the rate of carbon dioxide elimination and oxygen absorption. J. Clin. Invest. 11, 387–390 (1932).
-
Laster, M. J. et al. Visceral losses of desflurane, isoflurane, and halothane in swine. Anesth. Analg. 73, 209–212 (1991).
-
Fassoulaki, A. et al. Eger 2nd EI, Percutaneous loss of desflurane, isoflurane, and halothane in humans. Anesthesiology 74(3), 479–483 (1991).
-
Brunelli, A., Salati, M., Pompili, C., Gentili, P. & Sabbatinit, A. Intraoperative air leak measured after lobectomy is associated with postoperative duration of air leak. Eur. J. Cardiothorac. Surg. 52, 963–968 (2017).
-
Tsuboshima, K., Wakahara, T., Matoba, Y. & Maniwa, Y. Pleural coating by 50% glucose solution reduces postoperative recurrence of spontaneous pneumothorax. Ann. Thorac. Surg. 106, 184–191 (2018).
-
Zaraca, F. et al. Can a standardised ventilation mechanical test for quantitative intraoperative air leak grading reduce the length of hospital stay after video-assisted thoracoscopic surgery lobectomy? J. Vis. Surg. 3, 179 (2017).
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
This work was supported by JSPS KAKENHI Grant Number JP 22K08994.
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Asahi, T., Homma, T., Matsumoto, K. et al. Intrathoracic oxygen detects alveolar air leak following video-assisted thoracoscopic lung resection. Sci Rep 15, 31952 (2025). https://doi.org/10.1038/s41598-025-16882-w
-
Received:
-
Accepted:
-
Published:
-
DOI: https://doi.org/10.1038/s41598-025-16882-w