
Introduction
Wound management remains a persistent clinical and economic challenge1,2,3. Each year, more than 300 million surgical procedures result in acute wounds of varying complexity4,5,6, while the prevalence of chronic, non-healing ulcers increases as populations age and metabolic disorders such as diabetes become more common7,8. In high-income countries, these conditions contribute to healthcare expenditures amounting to billions of dollars annually1,3,9. Consequently, these challenges underscore the need for strategies that not only seal wounds but also support deep tissue regeneration for sustained therapeutic outcomes10,11,12.
Traditional sutures and staples have long served as the primary wound closure approaches due to their mechanical reliability and clinical familiarity11,12,13,14,15,16. However, they require specialized skills, can cause additional tissue trauma, and often lead to visible scarring. Emerging sutureless techniques have been introduced to address these drawbacks17,18,19,20,21,22,23,24,25,26,27,28,29. Laser-assisted sealing can help reduce scarring but requires precise energy delivery and specialized equipment18,19,20,21, whereas bioadhesives simplify application yet struggle to maintain stable tissue approximation under high tension22,23,24,25,26,27,28,29. Nonetheless, these mechanical approaches remain limited by the choice of materials, which can trigger inflammation, immune rejection, or delayed healing if lacking adequate biocompatibility. Consequently, both natural biomaterials (e.g., collagen, chitosan) and synthetic polymers (e.g., poly(lactic acid), polycaprolactone (PCL), polyvinyl alcohol (PVA), and polyurethane (PU)) have been extensively investigated to provide robust mechanical approximation, reliable biointegration, minimal cytotoxicity, and stable adhesion under physiologically moist conditions29,30,31,32. These material-related limitations, particularly inflammation and delayed healing, are further exacerbated in patients with compromised healing capacity, such as those of advanced age or with metabolic conditions, due to their inherently impaired immune responses and reduced regenerative ability7,8,30,31,32. Therefore, recent evidence indicates that achieving optimal therapeutic outcomes requires more than mechanical sealing, highlighting the need to carefully regulate the local tissue environment and prompting a shift toward more comprehensive wound management strategies33,34,35,36,37,38.
Integrative approaches that directly engage the cellular and molecular pathways governing wound repair, including pharmacological, protein-based, and biological strategies, have gained increasing attention33,34,35,38,39,40,41,42. Among these, electrical stimulation (ES), which mimics body’s endogenous electric fields38,39,40, has emerged as a promising technique. ES can enhance intercellular signaling and ion exchange, stimulate fibroblast proliferation, boost collagen deposition, and promote angiogenesis, thereby accelerating wound management and improving tissue quality3,4,41,42,43,44,45,46. These benefits are especially relevant for chronic or hard-to-heal wounds, offering a non-pharmacological means to expedite recovery and potentially reduce reliance on drug therapies47,48. Despite its promise, clinical implementation has proven challenging. Many ES systems rely on external power sources or implanted batteries, which increase device bulk, raise production costs, and generate additional waste, limiting feasibility in resource-constrained settings42,49,50,51,52. Additionally, the high impedance of human skin, often ranging from kilohm (kΩ) to megohm (MΩ) at low frequencies, together with impedance mismatches between the device and tissue can severely limit energy coupling and reduce electrical signal penetration, ultimately diminishing the therapeutic impact on wound healing53,54,55. Collectively, these challenges underscore the difficulty of developing a wound management platform that provides secure closure while also supporting key repair processes.
Herein, we present a sutureless, battery-free strip (SBF strip) that integrates mechanical stabilization and impedance-matched electrical stimulation in one biocompatible device. This platform offers four key advantages: (1) a near-body-temperature-responsive shape memory polymer (SMP) that contracts uniformly to ensure effective wound edge approximation; (2) strong wet-tissue adhesion, achieved through hydrogen and covalent bonding, enabling secure attachment to fragile or difficult-to-suture tissues; (3) a triboelectric energy harvesting (TEH) component, activated by ultrasound, providing impedance-matched high-frequency ES without external power sources; and (4) a flexible, cost-effective design that is both environmentally sustainable and easy to apply, ensuring compatibility with diverse clinical settings and requiring no specialized skills.
We employed a comprehensive stepwise approach that included finite element method (FEM) and computational modeling, experimental assessments of mechanical and electrical performance, and in vivo testing with rat models. Through this strategy, we demonstrated that the SBF strip can effectively approximate wound edges, provide sustained physiologically relevant ES, and accelerate tissue repair. Compared to conventional methods, it minimized scarring, enhanced epithelialization, and improved collagen deposition and angiogenesis. These findings highlight the SBF strip’s potential as a versatile and clinically adaptable wound management solution.
Results
Material and device design of the SBF strip
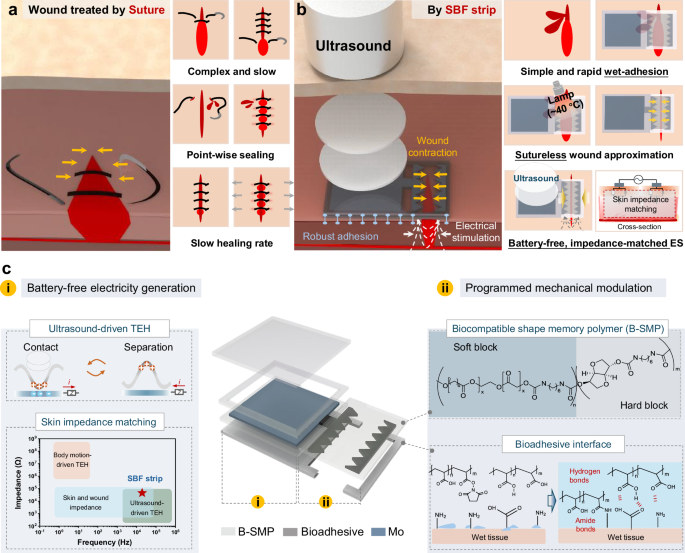
The SBF strip is designed for simplified fabrication and application, offering sutureless wound closure and battery-free ES for acute and surgical wounds (Fig. 1). When placed directly on the wound and gently heated to ~40 °C, its strain-programmed electrode contracts, pulling the wound edges closer and reducing stress concentrations for stable closure. To deliver ES, ultrasound (20 kHz) provides a controllable, high-frequency mechanical input to drive the TEH component at the tissue surface, enabling localized ES. At such frequencies, the device and skin impedances align within the kΩ–tens-of-kΩ range, facilitating efficient energy transfer and a uniform electric field53,54,55,56,57,58,59. Moreover, the adjustable output and wireless transmission capabilities of ultrasound allow the device to be customized for different wound types and patient needs, while extending its applicability to deeper tissues and internal organs, and ensuring a reliable energy source where mechanical motion cannot be readily harnessed (Fig. 1a–c).

Schematic illustrations comparing wound management with conventional suture treatment (a) to that with SBF strip (b). c Schematic of the device’s material structure and functionality, designed to achieve mechanical contraction and electrical stimulation. i. Battery-free electrical generation: Ultrasound-driven TEH converts contact-separation mechanical energy into electrical energy with efficient impedance matching skin and wound tissues. ii. Programmed mechanical modulation: The B-SMP’s shape-memory behavior and wet adhesive layer enable self-contraction and strong tissue bonding via amide and hydrogen bonds.
The SBF strip comprises three key materials: a biocompatible shape memory polymer (B-SMP), a bioadhesive layer, and molybdenum (Mo) foil (Fig. 1c, Supplementary Fig. 1). The B-SMP, a PCL-based PU, is pre-stretched to store elastic energy and contracts uniformly upon mild heating, enabling self-regulated wound closure without requiring specialized surgical skills. The bioadhesive layer, containing carboxyl and NHS ester groups, rapidly forms robust bonds on wet tissues via hydrogen and covalent linkages. Mo foil, serving as triboelectric electrode paired with the B-SMP triboelectric layer, efficiently converts ultrasound-driven mechanical vibrations into localized ES. Together, this integrated design provides a foundation for advanced, battery-free, and adaptable wound management strategies.
Sutureless mechanical modulation with wet-adhesive strain-programmed electrodes
The mechanical modulation of the SBF strip arises from compressive forces generated by its shape memory polymer (B-SMP) during thermal recovery and the strong adhesion to wet tissues (Fig. 2a). To ensure skin-safe deformation at near-body temperatures, we synthesized B-SMP from low-melting-point PCL diol via a one-shot bulk polymerization (Supplementary Fig. 2a). Its molecular structure was confirmed by 1H NMR (Supplementary Fig. 3), and the molecular weight was determined to be about 60,000 g mol−1 (Supplementary Fig. 4). Thermogravimetric analysis (TGA) revealed two major mass-loss events at 172.1 °C and 241.2 °C (Supplementary Fig. 5). Negligible degradation was observed when the film was immersed in phosphate-buffered saline (PBS) at 37 °C for 4 weeks, demonstrating good stability under potential physiological conditions (Supplementary Fig. 6). B-SMP’s shape memory behavior originates from its segmented block-copolymer structure, comprising chemically crosslinked hard segments (formed by hexamethylene diisocyanate and isosorbide) and soft segments (PCL-diol). These hard segments form a stable, permanent network that defines the polymer’s original shape. The PCL soft segments form reversible crystalline domains, which melt upon heating above their transition temperature, allowing temporary deformation. Cooling below this transition induces recrystallization, locking the polymer into its temporary shape. Upon reheating, the soft segments remelt, restoring mobility and enabling rapid recovery of the permanent shape, driven by the elastic memory in the crosslinked hard segments. With a Young’s modulus of 114 MPa, B-SMP achieves the mechanical robustness required for bioelectronic applications (Fig. 2b). Dynamic mechanical analysis (DMA) and differential scanning calorimetry (DSC) identified a glass transition temperature (Tg) of –10 °C and a melting temperature (Tm) of ~46 °C (Fig. 2c, Supplementary Fig. 7). Because room temperature ( ~ 25 °C) lies between these two transitions and far below Tm, the B-SMP remains in a stable, semi-crystalline state, preventing unintended shrinkage or spontaneous shape recovery after pre-stretching. Repeated shape memory cycle tests demonstrated a high recovery ratio of 91% (Fig. 2d). Supplementary Video 1 illustrates that a pre-stretched B-SMP film can recover its original shape within 2 seconds at 40 °C, highlighting its rapid thermal responsiveness. By combining pre-stretched B-SMP as the electrode substrate and unstretched B-SMP as the triboelectric layer, the electrode rapidly returned to its original dimensions upon heating, while the TEH component remained intact and functional (Supplementary Fig. 8, Supplementary Video 2).

a Schematic of strain programming and recovery in electrode substrate via thermally induced shape memory effects of B-SMP, with cross-sectional views depicting the adhesive mechanism to wet tissues. b Stress-strain curve of B-SMP at the room temperature. c DMA analysis of B-SMP: the storage modulus (E’), loss modulus (E”), and loss factor (tan δ). d Shape memory cycle test of B-SMP, illustrating the strain (%) and stress (MPa) as a function of temperature. The key phases of the shape memory process (deformation, fixing, unloading, and recovery) are annotated for clarity. e Quantitative evaluation of adhesion properties of the bioadhesive on wet porcine tissues (left, shear strength; right, interfacial toughness). Data represent mean ± SEM, with dots indicating individual measurements (n = 3 independent samples per tissue type). Statistical significance was assessed using one-way ANOVA (ns, not significant; exact P values are shown). f Quantitative evaluation of adhesion properties on moistened rat skin (shear strength and interfacial toughness), with dots representing individual measurements (n = 3 independent samples per group). g Images of SBF strips on wet tissues: heart, muscle, liver tissues. Scale bar: 1 cm. h Theoretical illustration of stress distribution around a skin wound (σ∞, pre-tension stress in intact skin; σwound, disrupted tensile stress at wound site; σr, radial stress; σθ, hoop stress; μ₀, skin shear modulus), complemented by representative finite-element simulation results.
To achieve reliable clinical performance, the SBF strip incorporates a wet-adhesive layer composed of covalently cross-linked poly(acrylic acid)-N-hydroxysuccinimide (PAA-NHS) and physically cross-linked PVA, forming an interpenetrating network (Supplementary Fig. 2b). Upon contacting moist tissues, hydroxyl groups from PVA and carboxyl groups from PAA-NHS/acrylic acid form hydrogen bonds with interfacial water and tissue surfaces, effectively removing interfacial water and providing immediate physical adhesion. Subsequently, NHS ester groups then covalently react with tissue amines to form stable amide linkages, ensuring robust and durable adhesion even in wet conditions25,26,30. Adhesion tests on ex vivo pig tissues using 180° peel (ASTM F2256) and lap shear (ASTM F2255) methods demonstrated rapid bond formation within 5 seconds (Supplementary Fig. 9), with shear strength over 70 kPa and interfacial toughness exceeding 200 J m−2 on heart, muscle, and liver tissues (Fig. 2e). Although slightly higher values were observed on liver tissue, no significant differences were observed among tissue types. It can also provide strong adhesion on moistened rat skins, with a shear strength of about 51 kPa and an interfacial toughness of about 131 J m−2 on the rat skin (Fig. 2f, Supplementary Fig. 10). With this bioadhesive layer, a simple 5-second application enabled the SBF strip to firmly adhere to fresh ex vivo pig tissues without detachment upon lifting with tweezers (Fig. 2g). By combining rapid shape memory response with strong wet adhesion, the SBF strip can swiftly adhere and deform, even under challenging in vivo conditions.
FEM simulations further clarified the SBF strip’s roles in modulating wound mechanics (Fig. 2h). Before the device is applied, the skin’s inherent pre-strain and tension concentrate stress at the wound edges. As the electrode starts to contract in response to mild heating, the simulation predicts a redistribution of these localized stresses, potentially guiding wound edges closer together without relying on sutures. By alleviating stress concentrations at this early stage, the model suggests that the SBF strip could create a more favorable mechanical environment for subsequent healing processes60,61. This capability to actively reshape local wound mechanics may inform future strategies that integrate biomechanical modulation with the underlying physiological repair processes.
Battery-free, skin impedance-matched electrical stimulation performance
In addition to providing mechanical closure, the SBF strip also integrates a TEH unit that enables battery-free, optimally skin-impedance-matched ES. Such impedance matching improves energy coupling and consequently enhances therapeutic efficacy. The TEH component comprises a B-SMP triboelectric layer and a Mo electrode (Supplementary Fig. 1). Driven by organ motion, human activity, or ultrasound, these layers undergo contact–separation cycles that generate triboelectric charges, thereby establishing an electric field on the wound surface. Among these driving mechanisms, ultrasound uniquely provides a controllable, stable high-frequency input suitable for optimized ES. To maximize ultrasound-driven ES, our SBF strip adopts a single-electrode configuration rather than the conventional dual-electrode design. Although this single-electrode configuration sacrifices the higher electrical outputs achievable with dual-electrode structures under low-frequency mechanical stimuli, it effectively reduces ultrasonic attenuation caused by the top electrode, significantly enhancing device performance specifically under ultrasonic excitation. Moreover, owing to the device’s robust bioadhesive interface, it adheres firmly to both superficial and deeper tissues, ensuring stable performance even in complex wound environments.
Another critical motivation for using ultrasound-driven ES lies in the inherent challenge posed by high skin and device impedances at lower frequencies, which severely limit the effective delivery of electrical signals into biological tissues under ordinary mechanical stimuli.
The capacitive properties of the epidermis can raise skin impedance to hundreds-of-kΩ or even MΩ, and most motion-driven triboelectric systems operating at low frequencies exhibit MΩ–GΩ output impedances (Supplementary Fig. 11), thereby reducing signal delivery and compromising therapeutic efficacy. To address these issues, we employ ultrasound as a controllable, high-frequency mechanical input. Operating at 20 kHz, ultrasound substantially lowers both the TEH device’s effective impedance and the skin’s impedance through high-frequency vibration, aligning their overall impedance in the kΩ–tens-of-kΩ range and thus enhancing ES penetration.
Next, we systematically evaluated the performance of our ultrasound-driven TEH component. The device was submerged in water, positioned 5 mm from the ultrasound probe (Supplementary Fig. 12a). Under 20 kHz ultrasound stimulation, the B-SMP membrane vibrated against the Mo electrode, producing consistent electrical pulses at the same frequency (Fig. 3a, Supplementary Fig. 13). At an ultrasound power of 0.5 W cm−2, it generated a peak voltage of 1.2 V (Fig. 3b) and a peak current of 19 µA (Supplementary Fig. 14), corresponding to an root mean square (RMS) voltage of 580.2 mV and an RMS current of 5.7 µA. The output voltage increased with the power density, reaching a peak of 1.81 V at 1.0 W cm−2 (E Supplementary Fig. 12b-d). By systematically varying the load resistance, we identified a maximum power density of 5.5 μW cm−2 at about 50 kΩ (Fig. 3c), indicating that at 20 kHz, the device’s effective internal impedance closely matches that of skin at high frequency. Although higher ultrasound intensities can enhance electrical output, intensities exceeding the safety threshold for diagnostic ultrasound recommended by the United States Food and Drug Administration (FDA) and the International Electrotechnical Commission (IEC) may introduce thermal or mechanical risks to biological tissues. Thus, based on both the established safety guidelines62,63, and insights from our previous ultrasound-driven triboelectric studies56,64,65, we selected 0.5 W cm−2 as the optimal ultrasound power density, ensuring effective electrical stimulation within a safe operational range. Supplementary Fig. 15 shows the SBF strip maintains a stable electrical output over 40 minutes of continuous ultrasound excitation at 0.5 W cm−2, with negligible fluctuations, confirming the reliability and durability of the TEH under sustained operation.

a Schematic illustration of the working principle of SBF strip under ultrasound stimulation, emphasizing membrane potential dynamics. The single-electrode-mode TEH component operates through four sequential contact-separation stages: i, Contact (initial charge transfer); ii, Equilibrium (charge stabilization); iii, Separation (triboelectric potential generation); iv, Equilibrium (restored charge balance). b Triboelectric voltage of SBF strip under 20 kHz ultrasound at 0.5 W cm−2, along with its zoomed-in waveform. c Load resistance analysis of SBF strip under the ultrasound (20 kHz, 0.5 W cm−2). d Acoustic pressure field and the total displacement of B-SMP film, triboelectric layer of device, set 5 mm from ultrasound probe underwater. e Surface potential of B-SMP before and after friction with Mo electrode. f Atomic modeling of triboelectrification of SBF strip denoting HOMOs. g Visualization of electron loss (blue) and electron gain (red) during triboelectrification. h Atomic analysis of charge transfer during triboelectrification.
To further elucidate the mechanical interaction responsible for the observed electrical outputs, FEM simulations show that ultrasound stimulation generates an acoustic pressure field, leading to microscale displacement within the B-SMP membrane (Fig. 3d). This displacement induces vibrations that facilitate contact with the Mo electrodes, thereby optimizing electro-mechanical coupling and electrical energy generation. Additionally, Kelvin probe force microscopy (KPFM) was used to validate the triboelectrification process by showing a 60.279 mV increase in B-SMP surface potential after friction with Mo, confirming electron loss from B-SMP during the process (Fig. 3a, e). For atomic-level interpretation of the triboelectrification phenomenon, we performed density functional theory (DFT)-based first-principles calculations. Figure 3f presents the atomic modeling of the contact model between B-SMP and Mo. The HOMO- and HOMO-1-consisting part of B-SMP (the urethane group) was used to represent the entire molecule, while Mo was modeled as α-MoO3, considering the native oxide layer of a few nanometers in thickness on the surface66,67. The details of the modeling each molecule are provided in Supplementary Figs. 16, 17, 18. The electron density difference around HOMO and HOMO-1 of B-SMP during contact is demonstrated in Fig. 3g and Supplementary Fig. 19, where blue and red domains represent the electron-donating and accepting parts. At the interface, B-SMP loses electrons while Mo accepts electrons, which is numerically analyzed by atoms in Fig. 3h, Supplementary Fig. 20. The results indicate the electron transfer occurs from B-SMP to Mo during triboelectrification and this finding aligns well with observed surface potential change and triboelectric series during friction (Supplementary Fig. 21). Further details of the DFT calculations and atomic analysis during triboelectrification are discussed in Supplementary Information. These DFT-based insights, combined with the KPFM measurements, confirm that electron transfer occurs from B-SMP to Mo during triboelectrification. In summary, ultrasound excitation drives the TEH system in a way that aligns its impedance with that of the skin, enabling a battery-free ES approach that effectively couples with biological tissues.
Electrical stimulation for cellular processes in wound healing
Building upon our previous demonstrations that the SBF strip, driven by ultrasound, can generate high-frequency continuous, impedance-matched triboelectric pulses, we next evaluated their impact on key cellular processes underlying wound healing, including cell migration and proliferation. During the device’s self-contraction, the distance between the serrated parallel electrodes decreased from 7 mm to 4 mm, and FEM simulations showed that it generated a high-frequency electric field of up to 0.59 kV m−1 under an ultrasound intensity of 0.5 W cm−2 (Fig. 4a). To assess the effect of these electrical signals on cell migration, we performed a scratch assay using fibroblasts cultured in serum-free medium. Microscopic images were taken at defined intervals, and the remaining scratch area was quantified using ImageJ, caculated as the percentage of the cell‑free region relative to the total image. After 16 hours, the control group retained a relative wound area of approximately 0.23, while the SBF strip-treated group reduced it to about 0.09, indicating significantly enhanced cell migration under electrical stimulation (Fig. 4b, c). In separate experiments evaluating proliferation, confocal laser scanning microscopy (CLSM) images of DAPI-stained fibroblasts at 48 hours revealed a notably higher cell density in the stimulated group (Fig. 4c), confirming that the high-frequency electric field also enhances cell proliferation.

a Cell migration and proliferation setup. Serrated electrodes positioned 4 mm apart, used for the SBF strip electrode in permanent state. Insets show FEM simulation of the electric field (Vpp = 1.2 V, 20 kHz). b Optical images of cell scratch experiment pre-stimulation (0 h) and post-stimulation (16 h). Scale bar: 100 µm. c CLSM images of fibroblast cells in proliferation experiments, with nuclei stained by DAPI. Scale bar: 50 µm. d Quantitative analysis of relative wound area reduction (top, cell migration assay) and cell proliferation (bottom, cell count per area) (mean ± SEM, n = 3 independent samples per group). e Schematic of the working process and mechanism of SBF strip to enhance the wound closure and healing processes. Here, σ∞ represents normal tensile stress in intact skin, σwound denotes the disrupted tensile stress at the wound site, and σf indicates contractile stress exerted by the self-contracting SBF strip.
Integrating these findings, we propose a mechanistic model for the SBF strip’s wound management approach (Fig. 4e). In healthy skin, epithelial cells maintain a transepithelial potential (TEP) of 25–50 mV, governed by ion gradients and Na+/K+-ATPase activity. Injury disrupts this TEP, generating a localized endogenous electric field critical in guiding cellular migration and repair3,4,42,43,46. Simultaneously, strain pre-load and stress concentration at the wound edges impede the natural healing process. The SBF strip addresses these challenges through a dual approach: its strain-programmed electrodes contract upon heating to realign wound edges and relieve mechanical stress, while the ultrasound-driven TEH generates high-frequency electrical pulses that overcome the capacitive barrier of the stratum corneum and penetrate deeper tissues. ES promotes wound healing by generating localized electric fields that alter cell membrane potentials and intracellular ion dynamics, subsequently activating critical signaling pathways involved in cellular proliferation and differentiation. Additionally, these localized electric fields guide the directional migration of key cells, such as keratinocytes, fibroblasts, endothelial cells, and macrophages, toward the wound site39,40,47,48. This directed cell migration further accelerates re-epithelialization, angiogenesis, and immune cell recruitment, collectively facilitating comprehensive tissue regeneration. By integrating impedance-matched high-frequency ES with mechanical approximation, the SBF strip significantly enhances energy transfer and promotes cellular activities, thereby expediting tissue regeneration, even in complex wounds.
Therapeutic effects of SBF strip for sutureless wound treatment
We next evaluated the SBF strip’s therapeutic efficacy in a rat surgical incision model. Prior to in vivo testing, MTT assays confirmed the biocompatibility of the newly synthesized B-SMP and the bioadhesive material, indicating no cytotoxicity over 72 hours, and cell viability comparable to untreated controls (Supplementary Fig. 22). Standardized acute cutaneous wounds were created in rats and randomly assigned to four groups (n = 5): (1) untreated control, (2) suture-only, (3) bioadhesive patch (no SMP contraction, no electrical stimulation), and (4) SBF strip (with SMP-induced contraction and triboelectric stimulation), as illustrated in Fig. 5a. Specifically, the bioadhesive patch served as a material-only control to confirm that improved wound healing resulted from the active contraction and ES provided by the SBF strip, rather than from the patch material’s intrinsic biological effects.

a Animal experiment setup and treatment protocol with SBF strip. b Snapshots of wound treated with SBF strip before and after lamp heating. c FEM simulation results to show the mechanical modulation on the skin surface and at 2.5 mm depth for an original wound and a SBF strip treated wound. (µ₀: shear modulus of the skin, σ/µ0: the normalized stress distribution). d Voltage output performance of SBF strip on rat skin under ultrasound (20 kHz, 0.5 W cm−2). e Sequential photographs of wound healing progress on Day 0, Day 1, Day 4, and Day 7 in various groups (n = 5). f Histological images of scar and wound tissues stained with Masson’s trichrome and CD31 immunostaining after 14 days. g Quantitative analysis of scar areas. Data are presented as mean ± SEM, with dots indicating individual data samples (n = 5 independent samples per group). Statistical analysis was performed using one-way ANOVA (exact P values are shown).
In both bioadhesive patch and SBF strip groups, pre-moistening the wound area ensured strong wet adhesion. In the SBF strip group, mild infrared heating raised the substrate temperature to ~40 °C, activating the strain-programmed shape-memory electrode substrate, and causing rapid, sutureless wound edge approximation (Fig. 5b, Supplementary Video 3). FEM simulations indicated that this contraction redistributed stress and reduced stress concentration around the wound site, extending up to 2.5 mm below the skin surface (Fig. 5c). Subsequently, the SBF strip group received a brief, 5-minute ultrasound input (0.5 W cm−2, 20 kHz) once daily for 4 days. After mechanical closure, low-intensity ultrasound stimulation triggered the SBF strip’s TEH component, generating high-frequency electrical pulses (Vpp ~ 1.1 V) that were delivered to the wound region through serrated electrodes (Fig. 5d). Because our primary focus was wound closure and ES-assisted healing, dynamically tracking changes in wound area were unsuitable; therefore, we relied instead on morphological observations over time combined with endpoint scar evaluation and histological analyses at Day 14 to comprehensively assess healing outcomes. After 24 hours, both the suture and SBF strip groups exhibited more pronounced wound closure than the remaining two groups. By Day 7, wounds treated with the bioadhesive patch and, notably, the SBF strip displayed advanced tissue regeneration and reduced scarring relative to the control and suture groups (Fig. 5e). This trend continued, and after 14 days, SBF strip-treated wounds showed the smallest scar areas, approximately 29.7% of the control and 38.3% of the suture group’s (Fig. 5f, g, Supplementary Fig. 23), which highlight the combined benefits of mechanical and electrical stimulation.
Histopathological analyses using Hematoxylin and Eosin (H&E), Masson’s trichrome, and immunohistochemical (IHC) staining for CD31 (an endothelial cell marker indicating angiogenesis) further illuminated tissue-level regeneration (Fig. 5f, Supplementary Figs. 24, 25). Whereas the control and suture groups exhibited marked inflammation and poorly organized collagen networks, the bioadhesive patch group showed moderate improvements. In contrast, the SBF strip-treated wounds surpassed all others by demonstrating abundant hair follicles, sebaceous glands, well-aligned collagen fibers, and robust angiogenesis, closely resembling physiologically normal skin architecture. Systemic safety evaluations showed no adverse effects. Histological examination of major organs (heart, liver, spleen, lungs, kidneys) detected no pathological abnormalities (Supplementary Fig. 25). Hematological and biochemical parameters, including Red Blood Cell (RBC) and White Blood Cell (WBC) counts, Alanine Aminotransferase (ALT), Calcium (Ca), and Creatinine (CRE) levels, remained within normal ranges (Supplementary Fig. 26), indicating no systemic toxicity. These findings suggest that the SBF strip poses minimal systemic risk while substantially improving wound healing outcomes.
Results and discussion
The SBF strip offers a robust, battery-free platform that unites mechanical wound approximation with impedance-matched ES in a single device. A shape-memory polymer (B-SMP) responsive to near-body temperature, combined with a rapid wet-adhesive interface ( > 200 J m−2), enables wound edges to be rapidly aligned, minimizing stress concentrations and promoting more uniform tissue repair. Ultrasound provides high-frequency (20 kHz) mechanical input to drive the TEH component, matching the device’s output impedance (~50 kΩ) with the skin’s capacitive properties (kΩ–tens-of-kΩ range). This synergy between B-SMP–mediated wound approximation and efficient ES delivery avoids reliance on external batteries. In vivo results demonstrate a 61.7% reduction in scar area compared with sutures, along with more organized collagen deposition and improved angiogenesis.
Many existing battery-free patches or stitches rely on low-frequency, motion-driven triboelectric harvesting. In contrast, our platform harness ultrasound-generated high-frequency mechanical inputs for optimized impedance matching (Supplementary Fig. 11), thereby enabling more uniform and enhanced electrical signal penetration. Critically, the synergistic combination of electrical stimulation and mechanical wound closure significantly accelerates treatment, enabling effective outcomes with brief daily interventions (~5 min/day) over several days rather than requiring prolonged or continuous application (Supplementary Table 1). This battery-free, wireless design not only simplifies the device architecture but also reduces maintenance demands and improves safety, particularly for deeper tissue injuries, internal wounds, or patients with constrained mobility, where conventional motion-driven or battery-powered systems can be cumbersome and pose additional clinical challenges (e.g., frequent recharging or heightened infection risks). Moreover, its sutureless configuration obviates the need for specialized expertise, making fabrication and clinical handling more accessible and cost-effective; together, these attributes highlight the SBF strip as a compact, portable, and practical solution for wound care, even in resource-limited settings. Building on these practical advantages, future studies would systematically evaluate the device’s performance in more complex clinical scenarios (such as chronic wounds and internal tissue regeneration), individually assessing the contributions of ES and mechanical contraction, and refining key parameters including ultrasound frequency, stimulation intensity, and treatment intervals. Such comprehensive research will ultimately expedite clinical translation, thereby significantly enhancing the accessibility and effectiveness of the SBF strip in clinical wound care practice.
Methods
Materials synthesis and film preparation
All chemicals were obtained from Sigma-Aldrich unless otherwise specified, and used without further purification. To synthesize B-SMP, PCL diol (19.82 g, 9.91 mmol) and isosorbide (1.45 g, 9.91 mmol) were added to a 100 mL round-bottom flask and stirred under N2 at 60 °C for 1 hour. Hexamethylene diisocyanate (3.33 g, 19.82 mmol) was then added, and the reaction was continued at 120 °C overnight via one-shot bulk polymerization. The synthesized polyurethane was dissolved in dimethyl formamide and precipitated in isopropyl alcohol as a non-solvent, followed by multiple washings for purification. The product was vacuum dried at 65 °C for 24 hours to obtain high-purity B-SMP. Subsequently, the B-SMP was dissolved in chloroform and then poured onto a glass plate to prepare a thin film with a thickness of 40 μm. To synthesize the Bio-adhesive, a precursor solution was prepared by dissolving 3.5 g of acrylic acid, 0.7 g of PVA, 0.1 g of PAA-NHS ester, 0.005 g of GelMA, and 0.02 g of α-ketoglutaric acid in deionized water. This solution was then poured into a custom-shaped PTFE mold with a spacer thickness of 200 μm. The mixture was cured under UV light (365 nm, 12 W) for 30 minutes. Finally, the cured adhesive was placed in a vacuum oven at 40 °C for 48 hours to remove residual water and unreacted small molecules for biocompatibility and long-term stability25,26,30.
Device fabrication
The fabrication process begins with laser structuring of Mo triboelectric and serrated electrodes, ensuring precise geometry for optimal energy harvesting. B-SMP, a PCL-based polyurethane selected for its low melting point ( ~ 46 °C) and superior adhesive properties, is laser-cut into the triboelectric layer, and pre-stretched as strain-programmed substrate. Mo electrodes are thermally bonded to the B-SMP substrate under controlled heating to ensure uniform adhesion. Subsequently, the bottom layer undergoes oxygen plasma treatment to enhance surface energy, followed by the application of a custom-molded bio-adhesive via thermal adhesion for robust mechanical and electrical integration.
Computational details
The calculation was carried out using DFT67,68 with generalized gradient approximation–Perdew–Burke–Ernzerhof (GGA–PBE)69,70,71 as an exchange–correlation functional, using the DMol3 code for HOMO analysis of B-SMP and CASTEP code for the contact electrification model of MoO3 and B-SMP. For the electronic property of SMP, all-electron methods were performed using atom centered basis set with double-numeric-plus-polarization, and at an orbital cut-off of 3.7 Å. The k-point was set to 1 × 1 × 1 gamma centered grid, which was used for the Brillouin zone sampling. The self-consistent-field (SCF) was converged in energy to 1 × 10−5 Ha, and direct inversion in the iterative subspace was used to increase the speed of SCF convergence. The structures were relaxed until the forces were less than 2 × 10−3 Ha Å−1. The molecular orbitals of SMP were mapped with an isosurface of 0.05 e Å−3. For the contact model between MoO3 and SMP, calculations were carried out using OTFG ultrasoft pseudopotentials. We used an energy cut-off for the plane wave of 630 eV and Monkhorst-Pack grid of 8 × 1 × 8 k-point meshes for the electronic calculations of MoO3 and 2 × 2 × 1 k-point meshes for the contact model of SMP and MoO3. The calculations were converged in energy to 10−6 eV cell−1 and the structures were allowed to relax until the forces were less than 3 × 10−2 eV Å−1. A vacuum layer of 12 Å was inserted perpendicular to the MoO3 slab to avoid spurious interlayer interactions.
FEM simulations
To quantitatively analyze the reduction in wound size and stress remodeling induced by SBF strip, we developed a three-dimensional finite element model using COMSOL Multiphysics 6.2. To facilitate computation and effectively display stress distribution, the model was appropriately simplified, focusing solely on the impact of the strain-programmed electrode part of SBF strip on the wound tissue. The human skin model used material properties from the COMSOL material library, with a Poisson’s ratio of 0.49 and a shear modulus of 40 kPa. Based on referenced settings (σ∞ = 0.17 µskin), the external stress on the skin was determined to be 6800 Pa30,72. The skin was applied with a 3.5% tensile pre-strain, and the parameters were set to 50 × 50 × 5 mm, density 1200 kg m−3, specific heat capacity at constant pressure 3391 J kg−1 K−1, and thermal conductivity 0.37 W m−1 K−1. The SMP was modeled as an incompressible Mooney-Rivlin hyperelastic material with parameters set to density 1109 kg m−3, and thermal conductivity 0.28 W m−1 K−1. The tensile pre-strain of the B-SMP was set to 30%. The initial temperature of the skin was set to 36 °C, with the bottom surface maintained at a constant 36 °C. The temperature field was configured to simulate heat transfer from an external heat source, aiming to raise the patch temperature to approximately 40 °C within 45 seconds, at which point the material begins to contract rapidly.
FEM simulations for ultrasound-driven SBF strip underwater were conducted using COMSOL Multiphysics 6.2. Physical parameters for water, Mo, and air were obtained from the COMSOL Multiphysics library, while mechanical and electrical properties for B-SMP were sourced from experimental data. The model involved a 1000 cm3 volume of water, with an ultrasound probe applying a load over a 3 cm diameter area and exerting a pressure of 5 × 105 Pa. This setup featured a device submerged in water, centered directly beneath the ultrasound probe. The device consisted of a top B-SMP film measuring 1.5 cm × 1.5 cm × 40 µm, a fixed bottom molybdenum electrode with dimensions of 1.2 cm × 1.2 cm × 25 µm, and a central air gap measuring 1.2 cm × 1.2 cm × 40 µm. Simulations incorporated pressure acoustics, solid mechanics, and acoustic-structure interaction to analyze the ultrasound at 20 kHz, examining its acoustic and mechanical interactions with the device components, as well as the membrane movement. The simulations did not account for mechanical contact between the membrane and the electrode.
Electrical characterization
In the study of the output performance of SBF strip under ultrasound, the device was submerged in water, positioned 5 mm away from an ultrasound probe with a diameter of 3 cm. The device was stimulated by 20 kHz ultrasound at varying power levels according to different experimental requirements. Voltage performance was measured and recorded using an oscilloscope (Tektronix DPO3052) with a voltage probe (Tektronix P5100A, 40 MΩ input impedance). Current signals were recorded using the oscilloscope and a low-noise current amplifier (FEMTO, DLPCA-200).
Ethics
All animal experiments were approved by the Institutional Animal Care and Use Committee (IACUC) of Samsung Medical Center (20230726001). Every experiment involving animals was carried out following a protocol approved by an ethical commission.
In vivo experiments
Female Sprague-Dawley rats (230–260 g) were purchased from Orient Bio (Republic of Korea). Animals were provided with standard chow and water ad libitum, and housed in a temperature-controlled (22 ± 2 °C), humidity-controlled (44–56%) environment with a 12 h light–dark cycle. Under isoflurane anesthesia (Hana Pharm Co., Ltd.), four acute skin incisions (1.5 cm in length, 0.5 cm width, 0.7 cm depth) were created on the dorsal skin of each rat. Animals were divided into 4 groups (n = 5 per group): (1) untreated control, (2) suture-only, (3) bioadhesive patch (no SMP contraction, no electrical stimulation), (4) SBF strip (with SMP-induced contraction and ultrasound-driven triboelectric stimulation). In both the Bioadhesive and SBF strip groups, the wound area was gently moistened with sterile gauze to provide a clean, hydrated surface, and gentle pressure (5–10 s) was applied to achieve immediate adhesion. For the SBF strip specifically, the TEH component was placed beside the incision, while the pre-stretched B-SMP electrodes were aligned along each wound edge (Fig. 5a, b). An infrared lamp (~40 °C) then activated the B-SMP, enabling self-contraction of the pre-stretched electrodes and suture-free wound closure. Ultrasound stimulation (0.5 W cm−2, 5 min/day) was administered for 4 consecutive days. Each device (bioadhesive patch or SBF strip) was replaced once daily during this intervention period due to photographic documentation and consistent performance. Rats were housed individually for realistic monitoring of device stability, and wound photographs were taken on Days 0, 1, 4, 7, and 14. In suture groups, non-absorbable interrupted sutures were applied following standard surgical protocols. To preserve consistent healing conditions, we determined that any wound reopening greater than 30% of its original length within the first four days would be reinforced with additional sutures. Throughout this period, however, no wounds exceeded this threshold, indicating stable closure. After the four-day intervention period, wounds healed naturally without further treatment. On Day 14, animals were euthanized, and wound tissues were harvested for histological analyses.
Histological and immunohistochemical analyses
Regarding H&E Staining, wound tissues and organs including heart, liver, spleen, lung and heart were harvested, fixed in 4% formalin for 24 hours, and embedded in paraffin. Paraffin-embedded tissue blocks were sectioned into 4 µm-thick slices using a microtome. The sections were deparaffinized in xylene and rehydrated through graded alcohols to water. They were then stained with hematoxylin for 5 minutes, rinsed in running tap water, differentiated in 1% acid alcohol, and rinsed again in water. The sections were counterstained with eosin for 2 minutes, dehydrated through graded alcohols, cleared in xylene, and finally mounted with a coverslip.
As for Masson’s Trichrome Staining, paraffin-embedded wound tissue sections of 4 µm thickness were deparaffinized in xylene and rehydrated through graded alcohols to water. The nuclei were stained with Weigert’s iron hematoxylin for 10 minutes and rinsed in running tap water. The sections were then stained with Biebrich scarlet-acid fuchsin for 15 minutes, differentiated in phosphomolybdic-phosphotungstic acid solution for 10 minutes, and stained with aniline blue for 5 minutes. After rinsing in distilled water and treating with 1% acetic acid for 3 minutes, the sections were dehydrated, cleared, and mounted with a coverslip.
In CD31 immunohistochemistry, paraffin-embedded wound tissue sections of 4 µm thickness were deparaffinized in xylene and rehydrated through graded alcohols to water. Antigen retrieval was performed by heating the sections in citrate buffer (pH 6.0) for 20 minutes. Endogenous peroxidase activity was blocked with 3% hydrogen peroxide for 10 minutes. Sections were then incubated with a primary antibody against CD31 (Abcam, ab182981, clone EPR17259; dilution 1:200) overnight at 4 °C. After rinsing with PBS, the sections were incubated with Goat Anti-Rabbit IgG H&L (HRP) (Abcam, ab205718; 1:200 dilution) for 30 minutes at room temperature. Color development was achieved using DAB substrate, and the sections were counterstained with hematoxylin, cleared, dehydrated, and mounted with coverslips.
Statistical and graphical analysis
Statistical analyses and graphing were performed using GraphPad Prism 9 (GraphPad Software), OriginPro 9.1 (OriginLab), and Microsoft Excel (version 16.0). One-way ANOVA was used to determine statistical significance, with significance levels defined as *P < 0.05, **P ≤ 0.01, ***P ≤ 0.001, and ****P ≤ 0.0001. Graphical illustrations and schematics were created using Microsoft PowerPoint, Rhino 7, and Figdraw.com (cartoon-style elements in Fig. 4e and Fig. 5a were created under academic-use permission).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All data supporting the findings of this study are available within the article and its supplementary files. Any additional requests for information can be directed to, and will be fulfilled by, the corresponding authors. Source data are provided with this paper.
References
-
Sen, C. K. et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 17, 763–771 (2009).
-
Dobson, G. P. Trauma of major surgery: A global problem that is not going away. Int. J. Surg. 81, 47–54 (2020).
-
Guest, J. F. et al. Health economic burden that wounds impose on the National Health Service in the UK. BMJ Open. 5, e009283 (2015).
-
Dare, A. J. et al. Global surgery: defining an emerging global health field. Lancet 384, 2245–2247 (2014).
-
Weiser, T. G. et al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet 385, S11 (2015).
-
Meara, J. G. et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet 386, 569–624 (2015).
-
Wicke, C. et al. Aging influences wound healing in patients with chronic lower extremity wounds treated in a specialized wound care center. Wound Repair Regen. 17, 25–33 (2009).
-
Armstrong, D. G., Boulton, A. J. M. & Bus, S. A. Diabetic foot ulcers and their recurrence. N. Engl. J. Med. 376, 2367–2375 (2017).
-
Olsson, M. et al. The humanistic and economic burden of chronic wounds: a systematic review. Wound Repair Regen. 27, 114–125 (2019).
-
Mangram, A. J., Horan, T. C., Pearson, M. L., Silver, L. C. & Jarvis, W. R. Guideline for prevention of surgical site infection, 1999. Hospital infection control practices advisory committee. Infect. Control Hosp. Epidemiol. 24, 250–278 (1999).
-
Yang, N., Venezuela, J., Almathami, S. & Dargusch, M. J. B. Zinc-nutrient element based alloys for absorbable wound closure devices fabrication: current status, challenges, and future prospects. Biomaterials 280, 121301 (2022).
-
Dunn, D. L. & Phillips, J. Wound closure manual. Ethicon, Somerville, New Jersey (2007).
-
Sobodu, O., Nash, C. M. & Stairs, J. 2024. Subcuticular suture type at cesarean delivery and infection risk: a systematic review and meta-analysis. J. Obstet. Gynaecol. Can. 46, 102191 (2024).
-
Burkhardt, R. & Lang, N. P. J. P. Influence of suturing on wound healing. Periodontol 2000 68, 270–281 (2015).
-
Steichen, F. M. & Ravitch, M. M. J. B. J. O. S. Mechanical sutures in surgery. Br. J. Surg. 60, 191–197 (1973).
-
Smith, T. O., Sexton, D., Mann, C. & Donell, S. Sutures versus staples for skin closure in orthopaedic surgery: meta-analysis. BMJ 340, c1199 (2010).
-
Taboada, G. M. et al. Overcoming the translational barriers of tissue adhesives. Nat. Rev. Mater. 5, 310–329 (2020).
-
Kramer, E. A. & Rentschler, M. E. Energy-based tissue fusion for sutureless closure: applications, mechanisms, and potential for functional recovery. Annu. Rev. Biomed. Eng. 20, 1–20 (2018).
-
Poppas, D. P. et al. Human albumin solder supplemented with TGF-β1 accelerates healing following laser welded wound closure. Lasers Surg. Med. 19, 360–368 (1996).
-
Fried, N. M., Walsh, J. T. Jr & Ravitch, M. M. Laser skin welding: in vivo tensile strength and wound healing results. Lasers Surg. Med. 27, 55–65 (2000).
-
Chen, Y., Wang, K., Huang, J., Li, X. & Rui, Y. J. C. R. I. B. An extensive evaluation of laser tissue welding and soldering biotechnologies: Recent advancements, progress, and applications. Curr. Res. Biotechnol. 8, 100234 (2024).
-
Wu, S. J. & Zhao, X. Bioadhesive technology platforms. Chem. Rev. 123, 14084–14118 (2023).
-
Topart, P., Vandenbroucke, F. & Lozac’h, P. Tisseel versus tack staples as mesh fixation in totally extraperitoneal laparoscopic repair of groin hernias: a retrospective analysis. Surg. Endosc. 19, 724–727 (2005).
-
Nam, S. & Mooney, D. Polymeric tissue adhesives. Chem. Rev. 121, 11336–11384 (2021).
-
Wu, J. et al. An off-the-shelf bioadhesive patch for sutureless repair of gastrointestinal defects. Sci. Transl. Med. 14, eabh2857 (2022).
-
Yuk, H. et al. Dry double-sided tape for adhesion of wet tissues and devices. Nature 575, 169–174 (2019).
-
Chansoria, P. et al. Instantly adhesive and ultra-elastic patches for dynamic organ and wound repair. Nat. Commun. 15, 4720 (2024).
-
Jin, S. et al. Injectable tissue prosthesis for instantaneous closed-loop rehabilitation. Nature 623, 58–65 (2023).
-
Li, J. et al. Tough adhesives for diverse wet surfaces. Science 357, 378–381 (2017).
-
Theocharidis, G. et al. A strain-programmed patch for the healing of diabetic wounds. Nat. Biomed. Eng. 6, 1118–1133 (2022).
-
Yi, J. et al. Rapid-response water-shrink films with high output work density based on polyethylene oxide and alpha-cyclodextrin for autonomous wound closure. Adv. Mater. 36, e2403551 (2024).
-
Blacklow, S. et al. Bioinspired mechanically active adhesive dressings to accelerate wound closure. Sci. Adv. 5, eaaw3963 (2019).
-
Zhu, J. et al. Smart bioadhesives for wound healing and closure. Bioact. Mater. 19, 360–375 (2023).
-
Baik, S. et al. Bioinspired adhesive architectures: from skin patch to integrated bioelectronics. Adv. Mater. 31, e1803309 (2019).
-
Hu, J. et al. Mechanically active adhesive and immune regulative dressings for wound closure. Matter 4, 2985–3000 (2021).
-
Wong, V. W. et al. A mechanomodulatory device to minimize incisional scar formation. Adv. Wound Care 2, 185–194 (2013).
-
Harn, H. I. et al. The tension biology of wound healing. Exp. Dermatol. 28, 464–471 (2019).
-
Gurtner, G. C. et al. Improving cutaneous scar formation by controlling the mechanical environment: large animal and phase I studies. Ann. Surg. 254, 217–225 (2011).
-
Zhao, M. Electrical fields in wound healing-An overriding signal that directs cell migration. Semin. Cell Dev. Biol. 20, 674–682 (2009).
-
Song, B. et al. Application of direct current electric fields to cells and tissues in vitro and modulation of wound electric field in vivo. Nat. Protoc. 2, 1479–1489 (2007).
-
Han, X. et al. Exosome-coated oxygen nanobubble-laden hydrogel augments intracellular delivery of exosomes for enhanced wound healing. Nat. Commun. 15, 3435 (2024).
-
Meng, X. et al. An ultrasound-driven bioadhesive triboelectric nanogenerator for instant wound sealing and electrically accelerated healing in emergencies. Adv. Mater. 35, 2209054 (2023).
-
Long, Y. et al. Effective Wound Healing Enabled by Discrete Alternative Electric Fields from Wearable Nanogenerators. ACS Nano 12, 12533–12540 (2018).
-
Du, S. et al. Self-powered and photothermal electronic skin patches for accelerating wound healing. Nano Energy 93, 106906 (2022).
-
Barman, S. R. et al. A self-powered multifunctional dressing for active infection prevention and accelerated wound healing. Sci. Adv. 9, eadc8758 (2023).
-
Luo, R. et al. Reshaping the endogenous electric field to boost wound repair via electrogenerative dressing. Adv. Mater. 35, e2208395 (2023).
-
Houghton, P. E. & Campbell, K. E. Choosing an appropriate wound therapy: electrical stimulation, ultrasound, and laser therapy. Adv. Wound Care. 12, 34–40 (1999).
-
Babaei-Ghazani, A., Eftekhar-Sadat, B., Arastoo, A. A., Talebi, G. & Goharpey, S. The effect of high-voltage pulsed current electrical stimulation on healing of pressure ulcers in patients with spinal cord injury: a randomized, single-blind clinical trial. J. Spinal Cord. Med. 42, 736–744 (2019).
-
Hannan, M. A., Mutashar, S., Samad, S. A. & Hussain, A. Energy harvesting for the implantable biomedical devices: issues and challenges. Biomed. Eng. Online 13, 79 (2014).
-
Won, S. M., Cai, L., Gutruf, P. & Rogers, J. A. Wireless and battery-free technologies for neuroengineering. Nat. Biomed. Eng. 7, 405–423 (2023).
-
Zhang, B. et al. A three-dimensional liquid diode for soft, integrated permeable electronics. Nature 628, 84–92 (2024).
-
Ates, H. C. et al. End-to-end design of wearable sensors. Nat. Rev. Mater. 7, 887–907 (2022).
-
Rosell, J., Colominas, J., Riu, P., Pallas-Areny, R. & Webster, J. G. Skin impedance from 1 Hz to 1 MHz. IEEE Trans. Biomed. Eng. 35, 649–651 (1988).
-
Rahimi, R. et al. A low-cost flexible pH sensor array for wound assessment. Nat. Biotechnol. 40, 402–412 (2022).
-
Song, J. W. et al. Bioresorbable, wireless, and battery-free system for electrotherapy and impedance sensing at wound sites. Sci. Adv. 9, eade4687 (2023).
-
Chung, Y. et al. Gigantic triboelectric power generation overcoming acoustic energy barrier using metal-liquid coupling. Joule 8, 2681–2695 (2024).
-
Hinchet, R. et al. Transcutaneous ultrasound energy harvesting using capacitive triboelectric technology. Science 365, 491–494 (2019).
-
Chen, C. et al. Micro triboelectric ultrasonic device for acoustic energy transfer and signal communication. Nat. Commun. 11, 4143 (2020).
-
Liu, X. et al. An ultrasound-driven implantable wireless energy harvesting system using a triboelectric transducer. Matter 5, 4315–4331 (2022).
-
Paul, M. D. Bidirectional barbed sutures for wound closure: evolution and applications. J. Am. Coll. Certif. 1, 51–57 (2009).
-
Chanda, A., Ruchti, T. & Unnikrishnan, V. Computational modeling of wound suture: a review. IEEE Rev. Biomed. Eng. 11, 165–176 (2018).
-
Souza, R. M., de Assis, M. K. M., Costa-Félix, R. P. B. & Alvarenga, A. V. Speed of sound in the IEC tissue-mimicking material and its maintenance solution as a function of temperature. Ultrasonics 118, 106564 (2022).
-
Moreno-Gomez, N., Athanassiadis, A. G., Poortinga, A. T. & Fischer, P. Antibubbles enable tunable payload release with low-intensity ultrasound. Adv. Mater. 35, e2305296 (2023).
-
Lee, D.-M. et al. An on-demand bioresorbable neurostimulator. Nat. Commun. 14, 7315 (2023).
-
Lee, D.-M. et al. Ultrasound-mediated triboelectric nanogenerator for powering on-demand transient electronics. Sci. Adv. 8, eabl8423 (2022).
-
Saji, V. S. & Lee, C. W. J. C. Molybdenum, molybdenum oxides, and their electrochemistry. ChemSusChem 5, 1146–1161 (2012).
-
De Castro, I. A. et al. Molybdenum oxides–from fundamentals to functionality. Adv. Mater. 29, 1701619 (2017).
-
Hohenberg, P. & Kohn, W. J. P. R. Density functional theory (DFT). Phys. Rev. 136, B864 (1964).
-
Kohn, W. & Sham, L. J. Self-consistent equations including exchange and correlation effects. Phys. Rev. 140, A1133–A1138 (1965).
-
Perdew, J. P., Burke, K. & Ernzerhof, M. Generalized gradient approximation made simple. Phys. Rev. Lett. 77, 3865–3868 (1996).
-
Perdew, J. P. & Zunger, A. Self-interaction correction to density-functional approximations for many-electron systems. Phys. Rev. B. 23, 5048–5079 (1981).
-
Pailler-Mattei, C., Bec, S. & Zahouani, H. In vivo measurements of the elastic mechanical properties of human skin by indentation methods. Med. Eng. Phys. 30, 599–606 (2008).Minor labeling corrections in Figure f for clarity. These changes are formatting only and do not affect the scientific content.
Acknowledgements
S.-W.K. acknowledges support from the Basic Science Research Program (2022R1A3B1078291, 2020R1A5A1019131) through the National Research Foundation of Korea (NRF) funded by the Korean government (MSIT).
Ethics declarations
Competing interests
X.M., X.X., S.J., D.K., B.-O.C. and S.-W.K. are inventors on a Korean patent application (application number: KR/10-2024-0156843), filed through the Office of Research Affairs/University Industry Foundation, Yonsei University. The patent relates to the self-contracting, battery-free triboelectric wound healing strip with strong wet adhesion described in this study. The other authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks Muhammad Ikram, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Meng, X., Xiao, X., Jeon, S. et al. Self-contracting, battery-free triboelectric wound healing strip with strong wet adhesion. Nat Commun 16, 7220 (2025). https://doi.org/10.1038/s41467-025-62312-w
-
Received:
-
Accepted:
-
Published:
-
DOI: https://doi.org/10.1038/s41467-025-62312-w