
Introduction
Soft and hard tissue defects resulting from periodontitis, trauma, or tumors significantly challenge natural tooth preservation and dental implant success1,2. Guided Bone Regeneration (GBR) and Guided Tissue Regeneration (GTR) are commonly used methods for regeneration and have shown excellent outcomes3,4,5. The fundamental concept of both treatments is to utilize barrier membranes to exclude non-target cells and promote the growth of target cells6,7. On the other hand, soft tissue augmentation techniques, which use autologous grafts or collagen materials to thicken or widen gingival tissue, are also widely employed to improve patients’ oral health8,9. However, the use of autologous grafts requires a secondary surgical site in patient’s mouth, while collagen materials are costly and may pose risks of immune rejection6,10. Therefore, there is an urgent need to develop alternative materials to address these challenges.
Platelet concentrates are widely used in tissue regeneration due to their excellent biocompatibility, as they are derived from the patient’s own blood11,12. Platelet-rich fibrin (PRF) is obtained through centrifugation of autologous blood, containing a natural fibrin scaffold, living cells, and growth factors13. Horizontal platelet fibrin (H-PRF), a novel type of PRF, is produced through horizontal centrifugation, which is a gentle centrifugation method that helps preserve the viability of the living cells14,15,16. When compressed into a membrane, H-PRF can be applied either alone or in combination with barrier membranes to cover bone substitute materials, or independently for soft tissue thickening or widening, all of which have demonstrated promising clinical outcomes17,18,19.
However, due to the rapid degradation of H-PRF membrane, it can only remain in the body with a typical duration of less than 14 days, which limits its application in tissue regeneration20,21. On the other hand, the mechanical strength of H-PRF membrane remains relatively low20,21, compromising its easy-handling and space-maintaining ability when used alone for hard and soft tissue augmentation20.
Since H-PRF is composed of inter cross-linked fibrin, it is desirable to utilize various physical or chemical methods to enhance the degree of fibrin cross-linking in H-PRF without disrupting the biological activity of growth factors20,22,23,24,25. Among the possible methods, tannic acid (TA) is a pentameric polyphenol structure that contains abundant phenolic groups that enable it to form chemical bonds with other materials as an active site26. It has been approved by the FDA of the United States and exhibits good biocompatibility, antibacterial and hemostatic properties when in contact with skin tissue26. Tahereh et al. found that tannic acid can improve the physical and mechanical properties of PRF gel without negatively affecting its biological properties27. However, the PRF gel treatment in this study requires a prolonged duration, typically overnight, which limits its clinical application. Therefore, the aim of the present study is to evaluate the potential and determine the optimal method of using tannic acid (TA) to crosslink platelet-rich fibrin (PRF) membranes at chairside, with the goal of improving their mechanical strength, degradation resistance, and antibacterial properties. The hypothesis is that TA treatment will yield PRF membranes with superior durability and antibacterial activity without compromising biocompatibility.
Materials and methods
Preparation of H-PRF
Blood samples were collected from eight volunteers, including three males and five females (average age of 25) after informed consent was provided. All the protocols used in this study were approved by the Ethics Committee of the School and Hospital of Stomatology, Wuhan University (B52/2020). All participants were in good health, were nonsmokers, had no symptoms of infection, and had taken no antibiotics for at least 3 months prior to the experiments. Then the blood was horizontally centrifuged at 700 RCF-max for 8 min in centrifugation (Plasmatrident, Weiyin Technology Co., Ltd., Wuhan, China)28,29. The upper yellow layer was H-PRF clot and was extracted from the tubes and compressed for 120 s using H-PRF preparation box (Plasmatrident, Weiyin Technology Co., Ltd., Wuhan, China) to acquire H-PRF membrane.
Cross-linking process
The previous study by Tahereh et al. showed that the TA solution at a concentration of 10% was not significantly cytotoxic to human fibroblast cells27. Therefore, tannic acid (TA) powder was dissolved in PBS solution to obtain the following concentrations of TA (0 mg/mL, 1 mg/mL, 10 mg/mL, 100 mg/mL), and the solution was filtered through a 0.22 µm filter for sterilization. H-PRF membranes were immersed in the TA solutions at different concentrations for varying durations (0 min, 1 min, 5 min, 10 min). Afterward, the membranes were removed from the TA solution and washed three times with sterile PBS to remove any unreacted materials.
H-PRF size and weight
Each H-PRF membrane was measured with a Vernier caliper and weighed after TA treatment. In the experiment, H-PRF and TA-PRF prepared using blood from the same donor were compared.
Mechanical strength testing
The mechanical properties of H-PRF membranes were measured using a tension meter (ZQ-990, ZhiQu). Prior to testing, freshly prepared membranes from each group were trimmed into rectangular strips measuring 20 mm × 10 mm (length × width) using a sterile scalpel, ensuring uniform sample size. Each strip was fixed between the grips of the testing device with a gauge length (distance between clamps) of 5 mm. The tensile rate was 1 mm/min and the maximum load capacity was 5 N under standard environmental conditions. The tension force and the corresponding tensile strain displayed by the tension meter during the stretching process were recorded. The stress was calculated by dividing the fracture force by the transverse section area of H-PRF membranes. The stress–strain curve was defined as ratio between the stress difference and the corresponding strain difference. Each group in this study was repeated with three replicates.
Scanning electron microscope
The H-PRF and TA-PRF samples were fixed at room temperature for 4 h with 2.5% glutaraldehyde (Merck, Darmstadt, Germany) and then dehydrated with gradient ethanol (25%, 50%, 75%, 100%) for 30 min at each concentration. Afterward, the samples went through critical point dehydration and gold sputter coating. The SEM images of surfaces and cross sections of these membranes were captured using a field emission scanning electron microscope (Zeiss, Sigma) under an accelerating voltage of 20 kV and a working distance of 7 mm. The magnification ranged from 2000 × to 6000 × at six different field views for each sample.
Quantitative measurements of fiber diameter and porosity were performed on representative high-magnification SEM micrographs using ImageJ software (National Institutes of Health, USA). For fiber diameter analysis, the image scale was calibrated based on the SEM scale bar, and the diameters of 4 randomly selected fibers per sample were measured using the straight-line tool. The mean diameter and standard deviation were calculated for each group. For porosity measurement, SEM images were converted to 8-bit grayscale and thresholded to distinguish fibers from void spaces. The images were then binarized, and the percentage of white (void) area relative to the total image area was calculated as the porosity. Measurements were performed on three independent samples per group, and the results are presented as mean ± standard deviation.
Bacterial preparation
The S. aureus (ATCC BAA-1758) and E. coli (MG 1655) strains were revived in LB broth overnight at 37 °C under aerophilic conditions. The optical density (OD) at 600 nm was measured using a microplate reader (PowerWave XS2; BioTek, Winooski, VT). The bacterial suspension was then diluted to 1 × 105 CFU/mL for experimental use.
Antibacterial test
1 membrane from each group was mixed with 4 mL of bacteria (1 × 105 CFU/mL) in 6-well plate and put on a shaking incubator for 2 and 6 h to investigate their antibacterial properties. Afterward, 100 µL of the sample was taken out and diluted with 900 µL of phosphate-buffered saline (PBS), then 30 μL of the mixture was plated onto an LB agar plate at 37 °C overnight for CFU counting. The antibacterial rate was calculated according to the following formula: Antibacterial rate (%) = CFU (PRF)—CFU (TA-PRF)/ CFU (PRF) × 100%. CFU (H-PRF) and CFU (TA-PRF) represent the mean colony-forming unit counts of the H-PRF and TA-PRF groups, respectively, at the same incubation time point.
Bacterial penetration test
The apparatus used for bacterial permeability experiment was prepared using the method described in the previous article30. Without destroying the sealing structure, the top of the lid of the 1.5 mL EP tube was perforated and sterilized, which was used as the inner chamber of the device. Each H-PRF membrane was cut into square with edge length of 1 cm. After adding 300 µL TSB medium to the inner chamber, the top of inner chamber was cover with trimmed H-PRF membrane, the plastic sealing clip was placed and the edge was secure with sterile plastic sealing film. After checking that the seal was intact, it was placed in the sterilized 50 mL centrifuge tube. 20 mL of TSB medium was added to the centrifuge tube as an outer chamber. The S. aureus cultures were diluted to OD600 = 0.1 and 200 µL bacterial suspension was inoculated into the outer chamber. The device was incubated in a 37 ℃ incubator. At 2 h and 24 h post-inoculation, culture medium from the outer chamber and inner chamber was taken to perform CFU counting assay. Ten microliters of liquid were spread onto TSB agar plate after series dilution. The plates were cultured in 37 ℃ incubator overnight. Bacterial penetration rate was determined using a two-chamber transwell assay, where the PRF or TA-PRF membrane was placed between the upper and lower chambers. After co-culture for the designated time points (2 h and 24 h), 100 μL of bacterial suspension from the lower chamber was serially diluted and plated for CFU counting. The penetration rate (%) was calculated according to the following formula: Penetration rate (%) = [CFU (outer chamber)—CFU (inner chamber)]/CFU (inner chamber) × 100%. CFU (outer chamber) and CFU (inner chamber) represent the mean bacterial counts in the lower and upper chambers, respectively, at the same time point.
Degradation test
After preparation, H-PRF membranes were placed in 6-well plates and incubated in a CO2 incubator at 37 ℃ with Dulbecco’s modified Eagle’s medium with 10% FCS and 1% antibiotics (Gibco, Thermo Fisher Scientific) to simulate the degradation processes occurring in vivo. The H-PRF clots were photographed and measured to track any changes in size or mass that occurred during the observation period.
Biocompatibility assay with human osteoblasts
Human osteoblasts (hFOBs) were purchased (LSMCE022). Cells between passages 2 and 5 were used for experiments. Briefly, 10 mL of whole blood was collected to prepare H-PRF membranes for each group. Following centrifugation, the upper layer of H-PRF was extracted and placed in a sterile culture dish containing 2.5 mL DMEM (HyClone, USA) and incubated at 37 °C for 24 h to obtain the H-PRF extract31. The supernatant was filtered and added to hFOBs culture medium at a 5% (v/v) concentration. Cells were seeded in 96-well plates at an initial density of 5 × 103 cells/well and cultured with hFOBs culture medium with H-PRF membrane extracts from different groups. Cell viability was measured at 1 and 3 days using the Cell Counting Kit-8 (CCK-8; Beyotime Biotechnology, China) according to the manufacturer’s instructions.
Statistical analysis
All experiments were performed at least in triplicate, and all data were presented as means with standard deviations (SD). Statistical significance was determined using one-way analysis of variance (ANOVA) followed by Tukey’s post hoc tests for pairwise group comparisons, with p values < 0.05 considered significant. All analyses were performed using GraphPad Prism 8.0 software.
Results
The appearance and the mechanical strength of crosslinked H-PRF
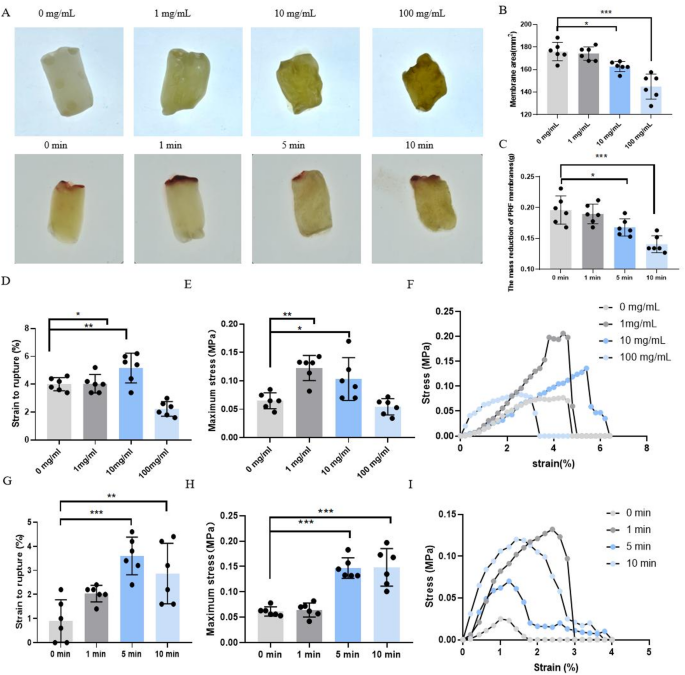
The appearance of TA-PRF membranes at different treatment concentrations and times, and the results of mechanical properties are shown in Fig. 1. It can be observed from Fig. 1A that the H-PRF membranes changed from a partially transparent gel-like to an opaque brown-yellow membranes after 10 min of treatment with a high concentration of TA. With the increase of H-PRF concentration, the maximum tensile strain increased gradually, but the concentration of 100 mg/mL decreased sharply. Although the maximum tensile stress of H-PRF membrane treated with 10 mg/mL concentration was lower than that of 1 mg/mL group, no significant difference was found. Therefore, the 10 mg/mL concentration was selected as the treatment group for subsequent experiments to evaluate the mechanical properties for different treatment duration. The results showed that both the maximum tensile strength and the maximum tensile strain of PRF membranes increased gradually with longer treatment times; however, no significant difference was observed between the 10-min and 5-min groups. Therefore, the shorter immersion time of 5 min was selected, as it provides comparable mechanical enhancement while offering greater clinical practicality by minimizing chairside preparation time.

Appearance and mechanical properties of H-PRF under different treatment concentrations and different processing times. (A) The photo of H-PRF membranes treated with crosslinking reagent. (B)The area of H-PRF membranes in different treatment groups. (C)The weight of H-PRF membranes in different treatment groups. (D, G)The strain to rupture of H-PRF membranes in different treatment groups. (E, H) The maximum stress of H-PRF membranes in different treatment groups. (F, I) The stress–strain curve of H-PRF membranes in different treatment groups. *p < 0.05, **p < 0.01, and ***p < 0.001.
The fibers structure of H-PRF and TA-PRF membranes
The structural features of the fibers before and after H-PRF cross-linking by SEM are shown in Fig. 2. It was observed that, before treatment with tannic acid (TA), the fiber bundles of the H-PRF were relatively thick, with a larger distance between the bundles. After treatment with TA, the fiber bundles became thinner and more densely packed. This suggests that the treatment with TA not only reduces the size of the fiber bundles but also enhances the compactness of the structure, potentially improving the overall mechanical strength and stability of the membrane. Quantitative SEM analysis showed that the mean fiber diameter of TA-PRF membranes was significantly greater than that of H-PRF controls (p < 0.05), while porosity was correspondingly reduced (Fig. 2E,F).

(A–D)Scanning electron microscopy images of horizontal platelet-rich fibrin membranes, scale bar = 2 µm(up) and 1 µm(down).(E)The fiber diameter of different groups. (F) The fiber porosity (%) of different groups.*p < 0.05, **p < 0.01, and ***p < 0.001.
Degradation of H-PRF and TA-PRF membranes in vitro
Over time, the H-PRF membrane dissolved in DMEM medium, but cross-linking using TA slowed down the degradation. In Fig. 3A, sequential photographic documentation at predefined time points provides a visual record of changes in membrane integrity and morphology during the degradation process. In Fig. 3B, we present quantitative measurements of residual membrane weight over time, allowing for kinetic analysis of the degradation process. At 28–35 day, TA-PRF retained greater residual mass than PRF (p < 0.001 and p = 0.00). Within groups, residual mass decreased from baseline (p < 0.001). These data indicate that TA modification prolongs membrane stability while maintaining structural integrity for an extended period.

Representative time-course degradation of H-PRF membranes. (A) The H-PRF membranes were cultured in Dulbecco’s modified Eagle’s medium with 10% FCS and 1% antibiotics (Gibco, Thermo Fisher Scientific). Each group was analyzed with three replicates. (B)The quality changes of different groups of H-PRF membranes. All the H-PRF membranes were cultured in Dulbecco’s modified Eagle’s medium with 10% FCS and 1% antibiotics (Gibco, Thermo Fisher Scientific). Each group was analyzed with three replicates. p < 0.05, **p < 0.01, and ***p < 0.001.
Antibacterial properties of H-PRF and TA-PRF membranes
Figure 4A, B present the quantitative antibacterial results for S. aureus and E. coli, respectively. Figure 4C presents the calculated antibacterial rates for both bacterial strains. After 2 h of co-culture, the CFU counts of S. aureus in the TA-PRF group were approximately 1.353E + 07, compared with 2.666E + 06 in the H-PRF group (p < 0.001), corresponding to an antibacterial rate of 79.995 ± 4.805%. For E. coli, the CFU counts were 2.617E + 06 in the TA-PRF group and 3.750E + 06 in the H-PRF group (p < 0.001), giving an antibacterial rate of 29.944 ± 13.295%. At 6 h, TA-PRF maintained significantly lower bacterial counts for both strains (p < 0.001), with antibacterial rates 98.037 ± 0.291% for S. aureus and 96.971 ± 1.950% for E. coli.

Quantitative analysis of S. aureus (A) and E. coli (B) bacterial colonies incubated with H-PRF or TA-PRF clots for 2 h and 6 h. (C) The calculated antibacterial rates. (D) The CFU counts showing the penetration fraction of S.aureus through membranes at 2 h,and 24 h. p < 0.05, **p < 0.01, and ***p < 0.001.
Bacterial exclusion ability of H-PRF and TA-PRF membranes
Figure 4D shows the bacterial penetration rates, defined as the percentage of bacteria that passed through the membrane from the outer to the inner chamber, at 2 and 24 h. At 2 h, both H-PRF and TA-PRF membranes exhibited low penetration rates, with TA-PRF slightly lower but without statistical significance. At 24 h, the penetration rate in the TA-PRF group (4.307 ± 0.8877) was significantly lower than in the H-PRF group (2.595 ± 0.575) (p < 0.01), indicating that TA modification enhances the membrane’s bacterial exclusion ability over longer periods.
Biocompatibility assay
As shown in Fig. 5, CCK-8 assays at both 1, 3 and 5 days revealed no significant differences in human osteoblasts (hFOBs) viability among the Blank and TA-PRF groups (p < 0.05). These results indicate that TA modification of H-PRF did not adversely affect the proliferation of human osteoblasts, demonstrating good cytocompatibility under the tested conditions.

The biocompatibility of H-PRF with or without cross-linking.
Discussion
When used as a membrane biomaterial, improving the mechanical properties and degradation profile of H-PRF is crucial for enhancing its clinical efficacy in guided bone regeneration (GBR) or soft tissue augmentation procedures. Improved mechanical strength facilitates space maintenance and allows for easier suturing and fixation of the membrane material, while an extended degradation period supports prolonged growth factor release and potentially enhanced barrier function. Given that H-PRF inherently exhibits relatively weak mechanical properties and rapid degradation, cross-linking to reinforce its fibrin scaffold may be a viable approach to improve its performance.
In this study, we found that soaking H-PRF membranes in 10 mg/mL TA solution for 5 min significantly enhanced the mechanical strength of H-PRF, supporting our previous hypothesis. Although this treatment caused minimal shrinkage in weight and surface area, the likely explanation is that TA induces platelet aggregation and promotes coagulation. The phenol groups in tannic acid may facilitate an interconnected fibrous structure and contribute to chemical activation within the blood. Quantitative SEM analysis confirmed that TA treatment produced a denser membrane structure, with significantly finer yet more tightly packed fiber bundles and reduced porosity compared with unmodified H-PRF. This microstructural densification likely reduces effective pore size, contributing to the improved bacterial exclusion ability observed in penetration assays. In parallel, TA-PRF demonstrated significantly enhanced antibacterial effects against S. aureus and E. coli, as shown by lower CFU counts and higher antibacterial rates at both 2 h and 6 h. The combination of direct bacterial suppression and physical exclusion provides a dual mechanism for infection control. Functionally, these microstructural and antibacterial improvements translated into superior mechanical stability and prolonged degradation time, both of which are clinically relevant for maintaining barrier integrity during regenerative procedures. The optimal treatment condition (10 mg/mL TA for 5 min) balanced mechanical enhancement, degradation resistance, and antibacterial efficacy while preserving biocompatibility. Indeed, CCK-8 assays on primary human osteoblasts showed no significant differences in cell viability between TA-PRF and control cultures at 1 and 3 days, indicating that TA modification is well tolerated by oral soft tissue cells. This comprehensive dataset underlines its promise as a membrane material capable of simultaneously enhancing mechanical durability, resisting bacterial infiltration, and maintaining tissue compatibility in periodontal and peri-implant regenerative applications.
Previous studies by our group have shown that thermal compression can reduce the surface area and porosity of PRF membranes and delay their degradation by up to 4 weeks32,33. Miron et al. found that heated preparation of Alb-PRF could prolong the absorption characteristics of liquid platelet-rich fibrin from 2 weeks to more than 4 months32,34. However, physical treatments may lead to random and heterogeneous cross-linking sites, which may reduce the stability of PRF if inappropriate conditions are used.
Other chemical cross-linking process were also investigated, including several types: aldehydes (formaldehyde, glutaraldehyde), carbonized diimines (EDC), double epoxides, cyanoisocyanates, etc35. Glutaraldehyde (GTA) is the most widely used reagent, which can reduce the antigenicity of collagen scaffolds. However, high concentration of GTA can reduce the biocompatibility of collagen materials and induce local cytotoxicity, which is not conducive to its application in vivo. One of the problems with the use of these types of chemical crosslinkers is their concentration dependent cytotoxicity, so the use of green crosslinkers such as genipin and TA may be a suitable alternative. Genipin can resist fibrinolytic degradation by forming covalent bonds with free primary amines32. After genipin treatment, the degree of enzymatic degradation (1%) of cross-linked PRF membranes was significantly lower than that of control samples. The lowest degree of degradation was observed after 72 h of treatment. In this study, TA was used as a crosslinking agent, requiring only a 5-min treatment time, making chairside crosslinking for immediate use a feasible option.
Although TA-PRF showed clear improvements in mechanical, degradation, and antibacterial properties, the lack of direct comparison with a benchmark commercial membrane remains a limitation. Literature indicates that while TA-PRF outperforms conventional PRF in these aspects, its degradation time (42 days) is still shorter, and its mechanical properties remain inferior, to those of widely used commercial membranes (e.g., Bio-Gide)36,37. Nevertheless, H-PRF offers unique biological activity and regenerative potential, which are well documented, and our aim was to enhance its clinical applicability—particularly as an adjunct to collagen membranes to boost biological activity or in soft tissue regeneration—rather than to fully replace collagen membranes at this stage. In future work, direct, quantitative comparisons with commercially available membrane under clinically relevant conditions is needed to further position TA-PRF within the context of established membrane performance standards.
Conclusion
In conclusion, TA modification of H-PRF membranes under the optimal condition (10 mg/mL for 5 min) enhanced mechanical strength, prolonged degradation, and improved antibacterial and bacterial exclusion abilities without compromising biocompatibility. These improvements highlight TA-PRF as a promising membrane for periodontal and peri-implant regeneration.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
-
Hammerle, C. H. F. & Tarnow, D. The etiology of hard- and soft-tissue deficiencies at dental implants: A narrative review. J. Periodontol. 89(Suppl 1), S291–S303 (2018).
-
Barone, A., Ricci, M., Tonelli, P., Santini, S. & Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implants Res. 24(11), 1231–1237 (2013).
-
Sculean, A., Nikolidakis, D., Nikou, G., Ivanovic, A. & Chapple, I. L. Stavropoulos a biomaterials for promoting periodontal regeneration in human intrabony defects: A systematic review. Periodontol.2000 68(1), 182–216 (2015).
-
Buser, D., Urban, I., Monje, A., Kunrath, M. F. & Dahlin, C. Guided bone regeneration in implant dentistry: Basic principle, progress over 35 years, and recent research activities. Periodontol.2000 93(1), 9–25 (2023).
-
Castro, A. B. et al. Regenerative potential of leucocyte- and platelet-rich fibrin. Part B: Sinus floor elevation, alveolar ridge preservation and implant therapy. A systematic review. J. Clin. Periodontol. 44(2), 225–234 (2017).
-
Mizraji, G. et al. Membrane barriers for guided bone regeneration: An overview of available biomaterials. Periodontol. 2000 93(1), 56–76 (2023).
-
Retzepi, M. & Donos, N. Guided bone regeneration: Biological principle and therapeutic applications. Clin. Oral Implants Res. 21(6), 567–576 (2010).
-
Thoma, D. S., Muhlemann, S. & Jung, R. E. Critical soft-tissue dimensions with dental implants and treatment concepts. Periodontol. 2000 66(1), 106–118 (2014).
-
Hammerle, C. H. & Giannobile, W. V. Working group 1 of the European workshop on p. biology of soft tissue wound healing and regeneration–consensus report of group 1 of the 10th European workshop on periodontology. J. Clin. Periodontol. 41(Suppl 15), S1-5 (2014).
-
Sheikh, Z. et al. Natural graft tissues and synthetic biomaterials for periodontal and alveolar bone reconstructive applications: a review. Biomater. Res. 21, 9 (2017).
-
Bianchi, S. et al. Platelets’ role in dentistry: From oral pathology to regenerative potential. Biomedicines 10(2), 218 (2022).
-
Blanco J, Carames J, Quirynen M. A narrative review on the use of autologous platelet concentrates during alveolar bone augmentation: Horizontal (simultaneous/staged) & vertical (simultaneous/staged). Periodontol 2000. 2024.
-
Miron, R. J., Fujioka-Kobayashi, M., Sculean, A. & Zhang, Y. Optimization of platelet-rich fibrin. Periodontol 2000. 94(1), 79–91 (2024).
-
Miron, R. J. et al. A novel method for evaluating and quantifying cell types in platelet rich fibrin and an introduction to horizontal centrifugation. J. Biomed. Mater. Res. A. 107(10), 2257–2271 (2019).
-
Li, H. et al. Liquid platelet-rich fibrin produced via horizontal centrifugation decreases the inflammatory response and promotes chondrocyte regeneration in vitro. Front. Bioeng. Biotechnol. 11, 1301430 (2023).
-
Feng, M. et al. Antibacterial effects of platelet-rich fibrin produced by horizontal centrifugation. Int. J. Oral Sci. 12(1), 32 (2020).
-
Hartlev, J., Spin-Neto, R., Schou, S., Isidor, F. & Norholt, S. E. Cone beam computed tomography evaluation of staged lateral ridge augmentation using platelet-rich fibrin or resorbable collagen membranes in a randomized controlled clinical trial. Clin. Oral Implants Res. 30(3), 277–284 (2019).
-
Pinto, N. et al. L-PRF in extra-oral wound care. Periodontol 2000. 97, 342 (2024).
-
Miron, R. J. et al. Use of platelet-rich fibrin for the treatment of periodontal intrabony defects: A systematic review and meta-analysis. Clin. Oral Investig. 25(5), 2461–2478 (2021).
-
Jia, K. et al. Platelet-rich fibrin as an autologous biomaterial for bone regeneration: Mechanisms, applications, optimization. Front. Bioeng. Biotechnol. 12, 1286035 (2024).
-
Sam, G., Vadakkekuttical, R. J. & Amol, N. V. In vitro evaluation of mechanical properties of platelet-rich fibrin membrane and scanning electron microscopic examination of its surface characteristics. J. Indian Soc. Periodontol. 19(1), 32–36 (2015).
-
Kardos, D. et al. Biological and mechanical properties of platelet-rich fibrin membranes after thermal manipulation and preparation in a single-syringe closed system. Int. J. Mol. Sci. 19(11), 3433 (2018).
-
Reksodiputro, M. H., Harahap, A. R., Setiawan, L. & Yosia, M. A Modified preparation method of ideal platelet-rich fibrin matrix from whole blood. Front. Med. 8, 724488 (2021).
-
Karimi, F. et al. Platelet-rich fibrin (PRF) gel modified by a carbodiimide crosslinker for tissue regeneration. RSC Adv. 12(21), 13472–13479 (2022).
-
Liu, X. et al. Genipin modified lyophilized platelet-rich fibrin scaffold for sustained release of growth factors to promote bone regeneration. Front. Physiol. 13, 1007692 (2022).
-
Marcinczyk, N., Gromotowicz-Poplawska, A., Tomczyk, M. & Chabielska, E. Tannins as hemostasis modulators. Front. Pharmacol. 12, 806891 (2021).
-
Haghparast-Kenarsari, T. et al. Improving properties of platelet-rich fibrin scaffold with tannic acid for wound healing. Int. Wound J. 21(4), e14571 (2024).
-
Fujioka-Kobayashi, M. et al. Histological comparison of platelet rich fibrin clots prepared by fixed-angle versus horizontal centrifugation. Platelets 32(3), 413–419 (2021).
-
Miron, R., Choukroun, J. & Ghanaati, S. Controversies related to scientific report describing g-forces from studies on platelet-rich fibrin: Necessity for standardization of relative centrifugal force values. Int. J. Growth Factors Stem Cells Dent. 1(3), 80 (2018).
-
Qiu, Y. et al. Bacterial exclusion and wound healing potential of horizontal platelet-rich fibrin (H-PRF) membranes when compared to 2 commercially available collagen membranes. Clin. Oral Investig. 27(8), 4795–4802 (2023).
-
Chai J, Chen Y, Shi S, et al. Efficacy of horizontal platelet-rich fibrin on gingival tissue regeneration: Cellular and histological analysis. J Periodontol. 2025.
-
Gheno, E. et al. In vivo evaluation of the biocompatibility and biodegradation of a new denatured plasma membrane combined with liquid PRF (Alb-PRF). Platelets 32(4), 542–554 (2021).
-
Yu, S., Wang, Y., Miron, R. J. & Zhang, Y. Structure, barrier function, and bioactivity of platelet-rich fibrin following thermal processing. Tissue Eng. Part C Methods 27(11), 605–615 (2021).
-
Miron, R. J. et al. 2024 extended platelet-rich fibrin. Periodontol 94(1), 114–130 (2000).
-
Giancola, C., De Sena, C., Fessas, D., Graziano, G. & Barone, G. DSC studies on bovine serum albumin denaturation. Effects of ionic strength and SDS concentration. Int. J. Biol. Macromol. 20(3), 193–204 (1997).
-
Kozlovsky, A. et al. Bio-degradation of a resorbable collagen membrane (Bio-Gide) applied in a double-layer technique in rats. Clin. Oral Implants Res. 20(10), 1116–1123 (2009).
-
Zhu, M., Duan, B., Hou, K., Mao, L. & Wang, X. A comparative in vitro and in vivo study of porcine- and bovine-derived non-cross-linked collagen membranes. J. Biomed. Mater. Res. B Appl. Biomater. 111(3), 568–578 (2023).
Acknowledgements
This work was supported by the National Natural Science Foundation of China (82170277) and Hubei medical youth top talent training program.
Patient consent statement
All participants provided informed consent prior to treatment on the study.
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
All the procedures carried out in this study were approved by the Ethics Commitee of the School and Hospital of Stomatology, Wuhan University (Number: B52/2020). All the procedures involving human participants have been performed in accordance with the Declaration of Helsinki. All participants signed informed consent before blood collection.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Y., Yu, S., Yang, W. et al. Tannic acid modified horizontal platelet-rich fibrin membrane with improved mechanical and biological properties for tissue regeneration. Sci Rep 15, 38233 (2025). https://doi.org/10.1038/s41598-025-22012-3
-
Received:
-
Accepted:
-
Published:
-
DOI: https://doi.org/10.1038/s41598-025-22012-3